 ARTAS Robotic System display monitor showing parameters for the creation of recipient sites
ARTAS Robotic System display monitor showing parameters for the creation of recipient sitesNew York, NY (PRWEB) — Robert M. Bernstein, M.D., F.A.A.D., A.B.H.R.S., founder of Bernstein Medical – Center for Hair Restoration, introduced new technology that allows the ARTAS Robotic System to accomplish a critical step in hair transplant surgery, the creation of recipient sites. Presenting at the 2nd ARTAS User Group Meeting, Dr. Bernstein previewed the recipient site creation technology that brings the robotic system one step closer to performing critical aspects of the labor-intensive, hair transplant procedure.
The ARTAS System is currently able to harvest intact follicular unit grafts from the permanent area in back of one’s scalp using precise robotic technology. This is the most difficult aspect of a follicular unit extraction hair transplant – the newer type of hair restoration procedure that avoids a linear scar in the back of the scalp. Now that site creation can also be done robotically, only one step remains – graft placement.
 The ARTAS Robotic System maps the surgeon’s hairline design onto a 3-D model of the patient’s head
The ARTAS Robotic System maps the surgeon’s hairline design onto a 3-D model of the patient’s headFor the recipient site creation, the doctor first draws a hairline and other markings directly onto the patient’s scalp to delineate the surgical plan. Next, multiple photographs are taken and fed into software, called the ARTAS™ Hair Studio, which converts the images into a 3-D model of the actual patient. This computer model can be manipulated and saved for the patient’s procedure. Using the ARTAS™ Hair Studio software, the physician then specifies the angle, direction, density, and randomness of the recipient site incisions to create the most natural look. During the procedure, the robot uses image-guided technology to avoid existing hairs while it creates up to 1,500 recipient sites per hour. In performing recipient site creation, the robot automates a process that can be physically demanding and prone to human error.
On the advancement, Dr. Bernstein said:
“This development is a crucial step towards a robotic system that can perform every aspect of a hair transplant. A great deal of credit goes to the engineers of Restoration Robotics who have worked to make automated recipient site creation a reality. I am proud that this work not only improves hair transplants for patients, but adds to the increasingly important trend of using robotic technology in medicine.”
The site creation technology that Dr. Bernstein debuted at the ARTAS User Group Meeting; which was held in California (Laguna Niguel, CA) on February 7th and 8th, 2014; will be available to hair restoration physicians in the fall of 2014. Gabe Zingeratti Ph.D, head of R&D at Restoration Robotics, Inc., presented details of the technology, which was beta-tested at Bernstein Medical – Center for Hair Restoration. With the next generation ARTAS® Robotic System rolling out in the coming months, the focus of research will then be on the final phase of robotic hair transplantation, the robotic insertion of follicular unit grafts into recipient sites. This last step will take several more years to develop.
The ARTAS Robotic System, developed by Restoration Robotics, is currently in use by hair restoration physicians around the world to automate the extraction of grafts of skin and hair called follicular units.. Follicular units, which are natural groupings of one to four hair follicles, form the biological basis of the modern hair transplant procedure. Once extracted from the back of the patient’s scalp, the follicular unit grafts are then inserted into recipient sites in the balding area of the scalp where they grow hairs that are immune to the effects of common hair loss.
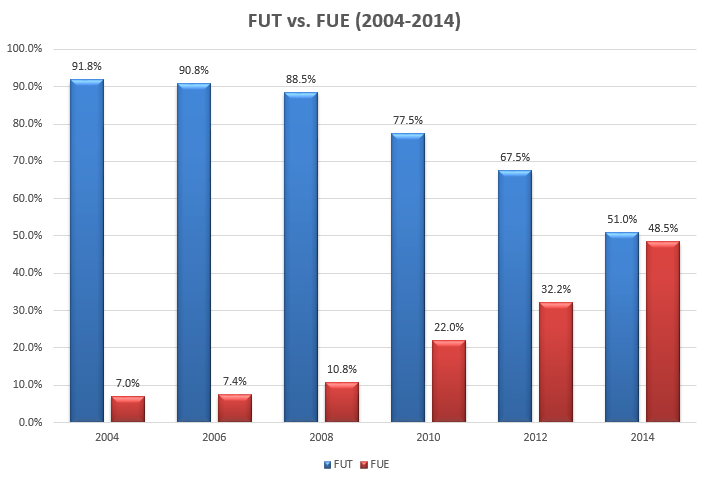
No stranger to innovative advances in hair transplant surgery, Dr. Bernstein introduced Follicular Unit Transplantation (FUT) to medical literature in a 1995 publication. FUT transformed hair transplants from the use of large grafts of skin and hair, known colloquially as “hair plugs,” to a more medically-oriented procedure that produces completely natural-appearing results. Dr. Bernstein with his colleague Dr. Bill Rassman again broke new ground with his 2002 publication that introduced the concept of Follicular Unit Extraction (FUE) to scientific literature. Dr. Bernstein was the first physician on the East Coast of the United Sates, and one of the first in the world, to use the ARTAS System to perform FUE using the new robotic technology.
About Robert M. Bernstein, M.D., F.A.A.D.
Dr. Robert M. Bernstein is a Clinical Professor of Dermatology at Columbia University and founder of Bernstein Medical – Center for Hair Restoration. His landmark scientific papers are considered seminal works in the field of hair transplant surgery. Other publications include textbook chapters on dermatologic surgery and books, like Hair Loss and Replacement for Dummies, aimed at the consumer audience. He has been selected as one of New York Magazine’s “Best Doctors” for fourteen consecutive years and has appeared as a hair loss and hair transplantation expert on The Oprah Winfrey Show, The Dr. Oz Show, Good Morning America, The Today Show, CBS News, Fox News, and The Discovery Channel. Dr. Bernstein has been interviewed or featured in articles in the New York Times, GQ Magazine, Men’s Health, Interview Magazine, Vogue, and others.
About Bernstein Medical – Center for Hair Restoration
Bernstein Medical – Center for Hair Restoration, founded in 2005, is a state-of-the-art facility and international referral center for the treatment of hair loss that is located in midtown Manhattan, New York City. Hair transplant surgery, hair repair surgery, and eyebrow restoration are performed using Dr. Bernstein’s pioneering techniques of Follicular Unit Transplantation (FUT) and Follicular Unit Extraction (FUE).
Posted by Robert M. Bernstein M.D. 

 The 21st Annual Scientific Meeting of the International Society of Hair Restoration Surgery was held in San Francisco from October 13 through 26, 2013. The meeting covers the most important scientific and clinical advances in the field of
The 21st Annual Scientific Meeting of the International Society of Hair Restoration Surgery was held in San Francisco from October 13 through 26, 2013. The meeting covers the most important scientific and clinical advances in the field of 



 New York, NY —
New York, NY —  Dr. Bernstein receives recognition from Restoration Robotics
Dr. Bernstein receives recognition from Restoration Robotics Dr. Bernstein discussing robotic-assisted FUE at Restoration Robotics’ first user meeting
Dr. Bernstein discussing robotic-assisted FUE at Restoration Robotics’ first user meeting
 The evolution of “follicular transplantation” can be attributed to three people. Dr. Robert Bernstein coined the phrase and advanced the concept. Dr. Bob Limmer ((Limmer B: Forum, Vol. 2, #2, 1991.)), ((Limmer B: J Dermatol Surg Oncol, 1994; 20:789-793.)) introduced the use of the binocular microscope, providing the technology, and Dr. David Seager showed by direct hair counts, comparing the growth of grafts cut with and without the microscope, how the hair growth was improved when the follicular unit was kept intact. ((4th Annual Meeting of the International Society of Hair Restoration Surgery September 19, 1996, “Does the size of the graft matter?”)), ((Seager, DJ: Micrograft size and subsequent survival — accepted for publication — Journal of Dermatologic Surgery.))
The evolution of “follicular transplantation” can be attributed to three people. Dr. Robert Bernstein coined the phrase and advanced the concept. Dr. Bob Limmer ((Limmer B: Forum, Vol. 2, #2, 1991.)), ((Limmer B: J Dermatol Surg Oncol, 1994; 20:789-793.)) introduced the use of the binocular microscope, providing the technology, and Dr. David Seager showed by direct hair counts, comparing the growth of grafts cut with and without the microscope, how the hair growth was improved when the follicular unit was kept intact. ((4th Annual Meeting of the International Society of Hair Restoration Surgery September 19, 1996, “Does the size of the graft matter?”)), ((Seager, DJ: Micrograft size and subsequent survival — accepted for publication — Journal of Dermatologic Surgery.)) I just returned from visiting Dr. Bob Bernstein in New York, and was impressed with his operation and even more impressed with his thoughts, observations, and insights into hair transplant surgery. He applies scientific methods to his work, is academically honest, and has an almost eerie instinctive knowledge of hair transplant surgery. Of course he has Dr. Bill Rassman to work with, but it is still remarkable. Dr. Bernstein is best known for introducing follicular transplantation ((R. Bernstein and W. Rassman Follicular Transplantation, International Journal of Aesthetic and Restoration Surgery. Vol. 3: No 2,1995, 119-132.)) to hair transplant surgery, an idea Bob Limmer has been pushing for ten years with the use of the binocular microscope, but no one would listen to him. Dr. Limmer, however, never used the term follicular transplantation. Using the microscope, you automatically dissect the follicular units. It can’t be avoided if done properly.
I just returned from visiting Dr. Bob Bernstein in New York, and was impressed with his operation and even more impressed with his thoughts, observations, and insights into hair transplant surgery. He applies scientific methods to his work, is academically honest, and has an almost eerie instinctive knowledge of hair transplant surgery. Of course he has Dr. Bill Rassman to work with, but it is still remarkable. Dr. Bernstein is best known for introducing follicular transplantation ((R. Bernstein and W. Rassman Follicular Transplantation, International Journal of Aesthetic and Restoration Surgery. Vol. 3: No 2,1995, 119-132.)) to hair transplant surgery, an idea Bob Limmer has been pushing for ten years with the use of the binocular microscope, but no one would listen to him. Dr. Limmer, however, never used the term follicular transplantation. Using the microscope, you automatically dissect the follicular units. It can’t be avoided if done properly.


