
Robert M. Bernstein, MD*,**, Robert McClellan, MD*, Roy Jones, MD*, Eugene Worton, MD*, Hendrik Uyttendaele, MD, PHD**
Dermatologic Surgery 2002; 28: 720-728.
*New Hair Institute Medical Group, A Professional Corporation, Los Angeles, California and **Department of Dermatology, Columbia University, College of Physicians and Surgeons, New York, New York
Introduction
MODERN HAIR transplantation began in the 1950s with an open donor method of harvesting using the “standard” 4mm punch based upon the pioneering work of Dr. Norman Orentreich. ((Orentreich N: Autografts in alopecias and other selected dermatological conditions. Annals of the New York Academy of Sciences 83:463-479, 1959.)) The size of the punch was gradually reduced in order to improve the survival of the hairs in the central part of the graft that had been subject to poor oxygenation (the donuting effect), and to make the hair transplant look more natural. Mini-micrografting, the use of large numbers of small grafts, harvested with a multi-bladed knife, rather than a punch, and then cut to the size the physician needed, became the standard for hair transplantation in the late 1980s and early 1990s. ((Rassman, WR, Carson S. Micrografting in extensive quantities. The ideal hair restoration procedure. Derm Surg 1995; 21:306-311.)) Follicular Unit Transplantation (FUT), a procedure in which hair is transplanted in its naturally occurring, individual follicular units, became state-of-the-art in the later half of the 1990s. ((Limmer BL: Elliptical donor stereoscopically assisted micrografting as an approach to further refinement in hair transplantation. Dermatol Surg 1994; 20:789-793.)), ((Bernstein RM, Rassman WR, Szaniawski W, Halperin A: Follicular Transplantation. International Journal of Aesthetic and Restorative Surgery 3:119-132, 1995.)), ((Bernstein RM, Rassman WR: Follicular Transplantation: Patient Evaluation and Surgical Planning. Dermatologic Surgery 23:771-784, 1997.)), ((Bernstein RM, Rassman WR: The Aesthetics of Follicular Transplantation. Dermatologic Surgery 23:785-799, 1997.)), ((Bernstein RM, Rassman WR, Seager D, et al.: Standardizing the classification and description of follicular unit transplantation and mini-micrografting techniques. Dermatologic Surgery 24:957-963, 1998.))
Punch harvesting was abandoned in favor of donor strip excision to maximize yield and minimize damage to the donor follicles. Punch harvesting became impractical for smaller grafts, as small changes in the incident angle of the punch transected proportionally more hair as the diameter of the punch was reduced. Generating grafts from a donor strip harvested with a multi-bladed knife was superior to the punch graft technique because it allowed in-vitro visualization of the tissue during the dissection process, but still caused a significant amount of transection. Precise control of graft dissection through direct visualization of the tissue was maximized using single-strip harvesting and stereo-microscopic techniques3. These techniques allowed for the removal of intact individual follicular units from the donor strip and were the enabling technologies for Follicular Unit Transplantation.
The only significant disadvantage to single-strip harvesting is the resultant donor scar. Although the scar usually heals as a nearly undetectable fine line, such a scar can potentially present cosmetic problems in patients who choose to wear their hair very short or in the rare individual who heals with a widened scar. Additionally, single strip harvesting can sometimes be problematic in patients with very tight scalps where a primary closure is difficult.
To circumvent the necessity of producing a linear donor incision, these authors began exploring variations of the punch technique. However, instead of using these punches to merely remove small pieces of hair bearing tissue, we have attempted to directly extract intact individual follicular units from the donor area without significant follicular transection; in effect, creating grafts that are identical to those generated by single-strip harvesting and stereo-microscopic dissection.
There are several problems inherent in removing individual follicular units with small punches. First, any significant variation between the incident angle of the punch and the exiting hair can result in graft transection. Keeping the punch parallel to the follicles throughout the entire length of the graft is difficult, as the visual cues used to guide one’s hand are lost once the punch passes into the depths of the tissue. Second, it is difficult to keep the punch perfectly oriented along a single axis when advancement into the tissue requires a back and forth twisting motion between the fingers. Third, the anatomic characteristics of follicular units are problematic for direct extraction.
Although it is now widely known that hair follicles in the human scalp grow in groups of 1-4 hairs, rather than as randomly spaced individual follicles, it is less well known that this grouping is a characteristic of the dermal component of the follicles only (Figure 1A). If one examines the subcutaneous layer of the scalp, one notes the distinctly random distribution of the bulbs ((Bernstein RM: A neighbor’s view of the “follicular family unit.” Hair Transplant Forum Intl. 1998; 8(3): 23-25.)) (Figure 1B). In order for follicles to be grouped on the surface of the scalp and be random in the fat, the follicles take a curved path through the skin. To visualize it another way, follicular units resemble a small bundle of wheat gathered at the top and splayed apart at the bottom.
The clinical implication of this is that a punch that neatly encompasses a follicular unit on the surface will amputate the splayed bulbs as it cuts through the deeper tissues. Our experience in trying to simply “punch out” follicular units with a small punch yielded results that would be anticipated from these anatomical considerations. It resulted in an unacceptable rate of transection (about 30%) with wide patient-to-patient variability.
In 1997, we began working on tools to circumvent the problem of follicular unit “splay.” Variations in instrument design, however, were not able to obviate the problem. Through correspondence with Dr. Richard Shiell in early 2001, it was brought to our attention that Dr. Masumi Inaba had described a unique process of removing hair from the donor area in which the punch was used to cut only part of the way down the follicle. The remainder of the follicle was then literally pulled from the scalp. A review of Inaba’s textbook produced an epiphany. It became clear that by cutting only partially into the dermis, many of the problems we were experiencing could be circumvented and transection could be reduced or eliminated.
We soon realized, however, that even with this “extraction” technique there was considerable patient-to-patient variability in obtaining intact follicular units. In some patients, follicular units could be removed completely intact. In others, the grafts pulled apart during their removal, resulting in the follicles being fragmented. We searched to find different hair characteristics that would account for this variability. The most obvious was hair shaft diameter. It was felt that thick, coarse hair would act to hold the graft together as it was extracted. It was also assumed that Inaba’s positive experience with the technique was based upon a select patient population, i.e., Japanese patients who characteristically have thick, coarse hair.
Unfortunately, the problem was not as straightforward as we had thought. Although successful extraction occasionally did correlate positively with hair shaft diameter, we found a number of Asian patients whose grafts fragmented during extraction and some fine-haired Caucasian patients in whom extraction was relatively easy. It was apparent that other factors were involved. It seemed that the dermis might be as important as the hair shaft in providing integrity to the graft during extraction. In conjunction with the Department of Dermatology of Columbia University, we began to study the donor tissue histologically to see what specific factors contributed to the integrity of the graft and could account for differences in their ability to be extracted.
We have defined Follicular Unit Extraction (The FOX ProcedureTM) as a technique of harvesting intact individual follicular units directly from the donor area using a small punch. In the procedure, a 1mm punch is placed directly over an individual follicular unit and, following the angle of the emergent hairs, the punch is passed partially through the dermis. Once the initial advancement is made, the bulk of the follicle is pulled with forceps, literally “extracting” the follicular unit from the scalp. It is important that the punch is small enough to leave an imperceptible donor scar.
The FOX TestTM allows the physician to determine which patients will be good candidates for the procedure. The FOX Test involves 5 or more small biopsies taken from the back of the scalp in the same manner as in The FOX Procedure. The extracted grafts are examined under a stereomicroscope for their integrity and/or sent for histologic examination.
This paper describes the FOX Procedure and the FOX Test, the indications for its use, and the limitations of the technique. It also attempts to explain why only select patients are good candidates for the technique.
Materials and Methods
The FOX Test
During the period of study, 200 consecutive patients undergoing their first follicular unit hair transplant procedure were asked to voluntarily undergo a Fox Test immediately prior to donor strip harvesting. After informed consent was obtained, biopsies were performed in the area where the donor strip was to be harvested.
The donor area was prepared for extraction by cutting the hair to a length of approximately 2mm with an electric clipper. This length was long enough to ascertain the hair direction, yet short enough that a 1mm punch could fit neatly over the tuft of hair arising from the follicular unit. Ring-block anesthesia was established using a mixture of lidocaine/bupivicaine/epinephrine. Local tumescence was established with a solution of Lactated Ringer’s. A 1mm punch was used for the biopsies. Between five and ten biopsies were taken from each patient. In select patients, a small section of intact donor strip was removed along with the punch biopsies and was submitted for histologic examination.
Each punch was advanced into the dermis (approximately 2mm), with care not to enter into the subcutaneous space. With experience, one can feel the increased resistance indicating that the punch had passed through the papillary dermis into the denser reticular dermis. If the resistance subsides, the punch has entered the subcutaneous space and has cut too deep.
After the punch incision was made, rat-toothed forceps were used to apply gentle pressure on the skin around the graft, elevating it lightly to allow the top part of the graft to be grasped. The amount of force (pull) needed to remove the graft varied from graft to graft and from patient to patient, although there seemed to be greater variability between patients than between grafts in the same patient. Care was taken not to tear the graft from the donor site, but rather to gently extract the graft out. If the graft was grabbed too close to the epidermal surface, pulled too hard, or too quickly, it tended to fragment. If the graft fragmented in spite of careful technique, it was scored as a negative test. Transection occurred if the surgeon was unable to keep the punch parallel to the upper portion of the follicular unit. The operator was usually able to adjust for this within the first few passes. If the problem persisted, then it implied a negative test result.
The extracted grafts were examined under a dissecting microscope to determine if the entire shaft came out intact. or if hair fragments were produced. They were then classified and sorted according to size (the number of presumed hairs contained in the original follicular unit). Biopsies were assessed on a scale of 1-5. A score of 1 was assigned when all of the follicular units were extracted intact. Patients who scored 2 had grafts that were extracted with most of the anatomy intact, but significant loss of the surrounding fat around the lower part of the follicle or some degree of amputation (< 20%) of the lower portion of the follicle. Patients who scored 4 had most of the surrounding fat avulsed with a significant number of distal follicles amputated. A score of 5 reflected significant damage in virtually all of the grafts with the upper portion of the follicles being avulsed from the lower segment in practically all of the samples. For clinical purposes, patients with positive FOX Tests were those classified as class 1 or class 2 and were considered potential candidates for the FOX Procedure. Those classified as class 3 were considered neutral (these patients might be considered positive if there was a strong indication to do the procedure). Those that were classified as class 4 or class 5 were considered FOX negative and not candidates for the FOX Procedure. The FOX Procedure
The FOX Procedure was performed on patients who were either FOX Test Class 1 or Class 2. The procedure is essentially identical to that of the FOX Test except that the organization of the larger procedure is more complex. The area that is needed for extraction is generally 8-10 times greater than the area needed for single-strip harvesting, with FOX Class 2 patients in the upper part of the range and FOX class 1 patients in the lower range, since the extraction is more efficient.
As an example, for a 500-graft extraction procedure, a donor area of approximately 50cm2 would be required in a FOX Class 2 patient and 40cm2 in a patient classified as Fox Class 1. With single strip harvesting, the same number of grafts would require 5cm2 (since the yield averages approximately 100 follicular units/cm2). This same 50cm2 area would yield only 200-300 intact follicular units in a FOX Class 4 or Class 5 patient, due to the excessive rate of transection. (Figure 2).
Results (Table 1)
Histological Examination
We investigated whether histological differences between hair follicles of FOX positive and FOX negative patients correlated with the observed clinical differences. Hematoxylin-eosin staining on scalp biopsies of 10 patients was performed.

 Figure 2. (A) Donor area 3 weeks post-op showing mild residual erythema. (B) Donor area 3 months post op.
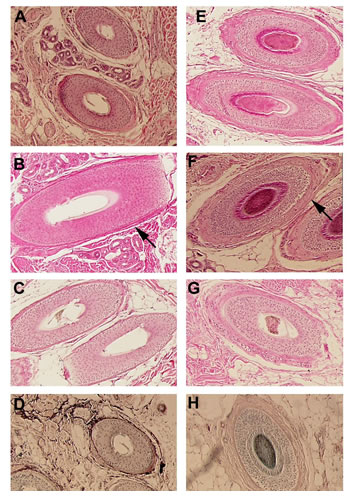
Figure 2. (A) Donor area 3 weeks post-op showing mild residual erythema. (B) Donor area 3 months post op.Five of the patients tested were classified as FOX positive (class 1) and five were classified as FOX negative (class 5).Histological analysis did not reveal any differences in the ratio of anagen versus telogen hairs between FOX negative and FOX positive patients. However a consistent difference in the thickness of the dermal sheath, which is a mesenchymal condensate that surrounds the hair follicle, was observed between FOX negative and FOX positive patients. FOX negative patients have a thicker eosinophilic dermal sheath surrounding the hair follicle (Figures 3 E-G), whereas 4 out of 5 FOX positive patients have a thinner dermal sheath (Figures 3 A-C). For this analysis we compared hair follicles of similar size and stage which were sectioned at a similar dermal depth as well as at a similar angle, in order to control for other factors that can influence the thickness of the dermal sheath.
To investigate whether qualitative differences within the dermal sheath may correlate with the observed clinical differences between FOX negative and FOX positive patients, we studied the elastin and smooth muscle content of the dermal sheath and associated fibroblasts. Orcein staining to detect elastin fibers reveals stronger and more prominent staining within the dermal sheath of FOX positive patients (Figure 2D) compared to FOX negative patients (Figure 3H). Immunohistochemistry using anti-smooth muscle actin antibodies did not reveal any significant differences in between FOX negative and FOX positive patients.
Discussion
Donor Wound Healing
In Follicular Unit Extraction, healing occurs by secondary intention, similar to the classic open donor method reported by Sasagawa (1930) ((Sasagawa M: Hair Transplantation. Jpn. J. Dermatol. 30:493, 1930 (In Japanese).)), Okuda (1939) ((Okuda S. Clinical and experimental studies of transplantation of living hairs. Jpn. J. Dermatol. Urol., 46: 135-138, 1939 (In Japanese).)), and Orentreich (1959)1. The major difference is the wound size. It is only the very small 1mm wounds of Follicular Unit Extraction that provide for rapid healing, produce an imperceptible donor scar, and offer a distinct advantage over the strip method with respect to donor healing.
Traditional Punch Grafting vs. Extraction
There are two different methods by which follicular units can be removed directly from the donor area using a punch. In the traditional way, the punch is used to cut the surrounding tissue the full length of the follicle. This can produce an unacceptable rate of transection due to the mechanical difficulty in keeping the punch aligned parallel with the hair follicles and from the splay of individual follicles as they enter the subcutaneous fat.
Inaba suggested a second method. He noted that after partial coring of the single-hair follicular unit, “the free composite hair is lifted with a pincette and its root is nipped with a very thin Pean’s forceps.” ((Inaba, Masumi Androgenetic Alopecia, Modern Concepts of Pathogenesis and Treatment, Springer-Verlag, Tokyo, 1996; pp 238-245.)) With that, the hair can be plucked out of the donor area once the graft has been freed at its base. Inaba’s insights were ingenious in that he identified that only the upper 1/3rd of the hair shaft needed to be cored and that traction could be applied to the hair follicle as it was pulled from its home position. The fact that he needed to have the root of the hair follicle “nipped” indicates that he didn’t realize that it was possible to pluck the hair completely out of the donor area in some patients.
The ability to “pluck” out a follicular unit without “nipping the base” varies with each patient. This is partially reflected in the FOX Test results discussed above. In patients who tested FOX positive, the yield was generally good and the surgery was efficient with the pull technique. In FOX negative patients, on the other hand, FUE was far more difficult to perform, was generally less efficient and had a high miss or transection rate.
Histology
The role of the dermal sheath in hair follicle development, growth and cycling is not well understood. It is possible that its function is to provide structural support to the hair follicle unit. We can only speculate if the observed differences in thickness and elastin content between FOX negative and FOX positive patients are related to the observed clinical differences.
Our findings, that the dermal sheath of FOX positive patients is thinner and more elastin-rich than those of FOX negative patients was surprising, as we had predicted just the opposite. We expected to find that FOX positive patients had a thick dermal sheath surrounding the hair follicle that would act as a support capsule and facilitate hair follicle unit integrity upon extraction.
The thicker dermal sheath actually observed in FOX negative patients may serve to anchor the hair follicle more tightly within the dermis and thus may prevent the follicular unit from being easily extracted. However, it is our clinical impression that this explanation is incorrect, since the tissue of FOX negative patients appears more friable and tends to pull apart during the extraction process, rather than causing increased resistance.
The hypothesis that the size of the dermal sheath is the determining factor, may be an oversimplification. It is likely that the molecular composition of the dermal sheath may be of much greater significance. It is possible that the higher elastin content, and consequently higher elastin/collagen ratio, found in the thin dermal sheaths of FOX positive patients may influence the possible anchoring function and/or possible support capsule function of the dermal sheath.
Patient Variability
We assessed a number of factors to explain patient-to-patient variability including hair shaft diameter, hair density, scalp tightness and race. There were no statistically significant correlations with these factors, but there was a tendency for patients with more coarse hair to display a greater degree of FOX positivity. As expected, Asian patients were more likely to be Fox positive than Caucasian patients. It was interesting, however, that some very coarse-haired Asian patients tested as low as a FOX class 4.
It is our impression that with a greater sample size (n value); a statistically significant correlation with some clinically observable hair characteristics will arise, with hair shaft diameter the most likely. It is obvious, however, that multiple factors are involved. In spite of the somewhat ambiguous histologic results, we have the strong clinical suspicion that dermal integrity plays a key role in FOX positivity and we will continue to pursue this area of research.
Not surprisingly, there was also variability within different parts of the scalp in the same patient. Hair direction can vary significantly within localized areas, as each follicular unit does not grow parallel to adjacent ones, even when the scalp is stretched with traction or tumescence. Because of this, the surgeon must continually monitor hair direction throughout the extraction procedure.
Transection
Dr. Inaba is of the opinion that when a hair shaft is transected, many of the follicles survive to produce a new hair11. It is important to keep in mind that Inaba focused upon single hair follicles and had no statistical scientific evidence to support his claims. If his assumptions are correct, then complete removal of the hair shaft is not critical. On the other hand, Dr. Kim has shown that although the amputated upper end of the hair shaft can regenerate a hair follicle (absent the distal third), the new hair follicle does not grow to the full diameter of its ancestor ((Kim JC, Choi, YC. Regrowth of grafted human scalp hair after removal of the bulb. Dermatol Surg 1995; 21:312-313.)). Therefore, it is reasonable to assume that if maximum fullness from a transplant is to be achieved, complete removal of the hair shaft and bulb is important in this new technique.
Follicular Unit Selection
Unlike strip harvesting, where every follicular unit in an area is removed, in the FOX Procedure the surgeon can select which units he wants to extract. Since the average Caucasian has approximately 30% 3- and 4-hair follicular units and 15% naturally occurring 1-hair units, one could select only the largest grafts when trying to achieve the greatest density, such as in the forelock region. In contrast, for eyebrow transplants, restoring temples, or refining the frontal hairline, the surgeon might select all 1- and 2-hair follicular units.
Donor Cosmesis
With follicular unit extraction, the prepped area presents a significant post-op cosmetic problem for two reasons: First, the area that needs to be accessed is much larger (8-10x as large), and second, the clipped area is not excised during the procedure, as it is in strip harvesting. To deal with this problem, the male patient is advised to have his hair either one of two lengths at the time of surgery. The ideal way for the patient to hide the harvested zone would be to grow the hair in the donor area long (longer than needed for strip harvesting) so that it would cover the wider shaved area. An alternative would be to cut all of the patient’s hair very short so that it would be essentially the same length as the harvested area. The wounds are generally not detectable after one week. By this time, the donor area blends in well with the surrounding scalp. The short-hair approach offers a much wider potential donor area for the FOX Procedure and may be a better choice for larger sessions.

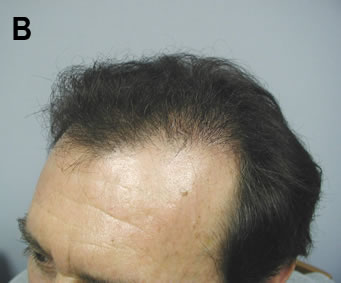 Figure 4. (A) 46 y/o Norwood Class 3 c/o temporal recession. (B) Six months after 2 sessions of follicular unit extraction spaced 12 days apart. A total of 743 follicular units were transplanted over the two sessions.
Figure 4. (A) 46 y/o Norwood Class 3 c/o temporal recession. (B) Six months after 2 sessions of follicular unit extraction spaced 12 days apart. A total of 743 follicular units were transplanted over the two sessions.Indications
In its present state, Follicular Unit Extraction has the following indications:
• People with limited hair loss or those who require small sessions. This group would include patients with androgenetic alopecia in a Norwood Class 3 pattern or those with small vertex balding areas (Figure 4)
• Limited cosmetic areas, such as widow’s peaks, eyebrows, eyelashes, mustaches
• Alopecia secondary to dermatologic conditions
• Scarring from dermatologic conditions, trauma, or neurosurgical procedures
• Individuals with low donor supplies, heavily scarred donor areas or very tight scalps
• Patients who tend to heal with wide scars
• Select repairs
• Those who wear their hair very short
• Athletes who must resume full activity soon after the procedure
With further experience with this technique, we expect these indications will be modified and new indications will be found.
Conclusion
Follicular Unit Extraction is a minimally invasive surgical procedure that can benefit a limited subset of patients in a hair restoration practice. The FOX Procedure involves the direct extraction of the follicular units from a patient’s donor area using a small punch. At this time, approximately 60% of patients are candidates for this procedure, and the procedure itself is practical in individuals who require less than 600 grafts at a sitting. Healing is quick, scarring is virtually nonexistent, and discomfort in the donor area has been virtually eliminated. The authors believe that Follicular Unit Extraction can benefit select patients and should be available in every hair restoration practice for use in appropriate candidates.



