
Robert M. Bernstein, MD, New York, NY
William R. Rassman, MD, Los Angeles, CA
Dermatologic Surgery 1997; 23(9): 785-799.
The recent trend in hair restoration to perform larger sessions has had the tendency to shift the surgeon’s focus from the aesthetic aspects of the procedure to the simple gratification of transplanting ever increasing numbers of grafts. The ability to transplant extensive quantities of follicular implants has added great power to the transplant procedure. However, its ultimate value lies not in absolute numbers, but in its ability to be of cosmetic benefit to the patient. There are a host of subtle nuances, which, when used properly, can transform the procedure from one that merely decreases the number of operations, to one that allows the surgeon to more closely approximate the natural appearance of the patient’s original hair.
The concept and technique of “Follicular Transplantation” has been described by these authors in a 1995 publication ((Bernstein RM, Rassman WR, Szaniawski W, Halperin AJ. Follicular transplantation. Int J Aesthet Rest Surg 1995; 3:119-132.)). This article focuses on areas in which the physician’s aesthetic judgments are critical to its successful outcome. (Please refer to reference 1 for a more detailed description of Follicular Transplantation and its glossary for the clarification of specific terms. In addition, it is important to be familiar with the Norwood Classification ((Norwood OT. Male pattern baldness: classification and incidence. So. Med. J 1975;68:1359-1365.)) of male pattern baldness, as this will be used frequently in the following text.)
Hair Distribution
Density
An average scalp is approximately 500 cm2 (50,000 mm2). Since the normal, non-balding scalp has 1 follicular unit/mm2, and each unit contains on the average 2 hairs (yielding a density of 2 hairs/mm2), the average scalp would have 100,000 hairs in total. The permanent zone normally represents approximately 25% of this area, and half is available to be moved without the donor area appearing too thin. Thus, in theory, 12.5% of the scalp would be available for transplantation. This donor area would contain 12,500 hairs or 6,250 implants, averaging two hairs each. When a patient’s density is higher, a greater proportion of the donor hair can be used for the transplant (see ref. 1, table 1).
Simple arithmetic reveals that only 12.5% of the scalp would normally be available to cover the remaining 75% that could become bald. In these computations, the potentially bald area thus represents a surface 6 times as large as the donor area. If all the available donor hair was transplanted, with no loss of hair from the harvesting and dissecting of the implants (which of course is not possible), and the implants were uniformly spaced, this would produce a recipient density of at most 17% of the original density. In the first session, in a person with a scalp of average laxity, a maximum of approximately 50 cm2 may be harvested from the donor area, achieving a maximum density of only 13% of the original. A second procedure can increase the density in the previously treated balding area somewhat, but the amount that can now be harvested due to the lowered density and tighter scalp will be less, and the aesthetic benefit will be proportionately less dramatic. If we attempt to increase the density by increasing the size of the implants, the ratio becomes worse. Doubling the size of the follicular unit (by combining two units together) will increase the spacing between them to a ratio of 1 to 12 (and produce a less natural appearance), but this will not change the overall recipient density which will remain at 17%.
These numbers are not as dismal as they appear. In a completely bald area, 17% of the patient’s original density offers a vast cosmetic improvement over having no hair, especially if the transplant is totally natural, and the patient has realistic expectations. But most importantly, the aesthetic impact of these absolute numbers can be improved upon with “artistic” adjustments in the “weighting” of the implants. In addition, if it can safely be assumed that the patient will not be extensively bald, then more hair can be committed to a more limited area. Great care must be taken so that excessive amounts of hair are not removed from the donor area to treat a limited area of recession, given the possibility that such a patient may need to reserve his donor hair to cover an almost certain evolving hair loss process over time.
The decision regarding moving hair reserves to meet patients goals must be a joint one between patient and doctor. The doctor has the obligation to fully inform the patient of the consequences of donor hair depletion when planning any reconstruction.
We feel that the solution to increasing recipient density should be to perform a properly planned second procedure using follicular units and not to increase the size of the implants, since this will result in a density that is either equal to or greater than (due to compression) the density of the donor area. This density will either be unnatural for a mature patient whose density in the front and top of his scalp should be less than in the donor area, or unrealistic if future hair loss should occur (and this level of density cannot be maintained). Conversely, splitting up the follicular units would not increase the density either. This would only produce groupings smaller than occur naturally and would run the risk of having poor growth and an appearance that was too thin.
The question often arises regarding how close grafts can be placed and still achieve maximum viability. Graft survival is largely dependent upon maintaining intact follicular units in the dissection, and then taking meticulous care of the units throughout the implantation process, rather than being related to the spacing of the sites per se. The sites used in the follicular transplantation process are so small (1.0 to 1.5 mm) that injury to the recipient area is very limited. Under normal circumstances, we find that this allows for unhindered growth at the densities described above. The close placement of follicular units is a mechanical problem related to the bulk of the implant, the size of the site, the distensibility of the scalp, and the ability to control hemostasis (we do not recommend the use of lasers to control hemostasis as it will cause unnecessary destruction of the skin in the recipient area ((Bernstein R, Rassman W. Laser hair transplantation: is it really state of the art? Lasers in Surg and Med 19:233-235, 1996.))). The close placement of implants can be achieved by the coordinated efforts of a highly trained surgical team skilled in this technique. The degree to which grafts may be safely placed together, however, is not unlimited. We exercise more caution in the close placement of recipient sites under the following circumstances:
- when there is recipient site scarring (i.e. from scalp reductions or punch grafting)
- when there is marked actinic damage (solar elastosis) in the recipient area
- when there are hyperfibrotic changes in the recipient area
- with the scalp atrophy and decreased vascularity seen in long-standing baldness
- if the patient has an underlying medical condition that may retard healing (such as diabetes)
- when the patient uses drugs, such as tobacco, which interfere with the normal healing process.
Weighting
For simplicity, the balding portion of the average person’s scalp can be divided into three regions:
1) The frontal portion comprises the frontal hairline and the area immediately behind it. It is bounded posteriorly by a line drawn from the point where the frontal hairline forms an acute angle with the temple, to the corresponding point on the other side. It roughly measures 50 cm2. 2) The top of the scalp, which lies immediately behind the front and extends to the crown. The hair in the top portion of the scalp points in a forward direction. It includes the vertex, which is the most posterior part of the top and is the highest part of the skull. Its surface area is about 150 cm2. 3) The crown, which is defined as the portion of the scalp behind the vertex, where the hair takes on a swirling pattern. It has poorly defined lateral and posterior boundaries but can assume a size of about 175 cm2 or more in a Norwood Class VI/VII patient, although crown size can vary widely (figure 1A).
In general (assuming straight, brown hair of average hair weight, and light skin), 50% of the hair in a given area may be lost before any appreciable change is noted. For the average person, with a density of 2.0, this would result in a density of 1 hair/mm2. This might be considered the “ideal” density after a transplant, since anything above this would be unnecessary and, of course, in a balding patient, substantially less may be adequate, especially with better-than-average hair characteristics. A typical Norwood Class VI patient might require about 2,500 follicular units to cover the front and top of the scalp (5,000 hairs over 200cm2), leaving the crown bare. If implants containing on average 2 hairs each are evenly distributed, this would result in a density of 0.25 hairs/mm2, or 25% of the “ideal” transplant density of 1 hair/mm2 (figure 1B). If, however, 1000 units were placed in the front 50 cm2, then this density would be 0.4 hairs/mm2 or 40% of the ideal density. The remaining 150cm2 could be transplanted with 1,500 implants for a density of 0.2 hairs/mm2 or 20% of the ideal density. This distribution is referred to as “forward weighting” (figure 1C).
Since most people are seen from a frontal or ¾ view, the overall appearance of the patient described above is essentially defined by the density of this frontal area. A second procedure could then approach 80% of the ideal density (or 40% of the original density) in limited areas and would, in most cases, produce a final cosmetic result that was completely satisfactory. This, of course, assumes that there is enough scalp laxity for a large second procedure and that the crown has not been transplanted. When a patient has higher density, good hair quality (such as coarse or wavy hair), or low skin/hair color contrast, this may compensate to some degree for the tighter scalp, although a tight scalp can be an important factor limiting the yield in subsequent surgeries. If all the elements for an excellent transplant are not present, very satisfactory results can still be achieved as long as more conservative goals are established beforehand. Crown coverage can be accomplished in a number of situations, and these are discussed in the section on “goals for the second session.”
Another means of weighting the transplant is to concentrate larger follicular units in the more important cosmetic areas. This can be used with an even distribution of sites or be superimposed upon an already “weighted” distribution (figure 1D). Forward weighting in combination with the central placement of larger follicular units is the most common distribution that we use and is illustrated in the case study that follows this text. We “forward weight” the distribution of the sites to enhance the frontal view, and then use larger follicular units in the mid-portion of this area to create more central density. The use of the larger units will produce more weighting closer toward the midline in a “forelock type” distribution. The advantage is that you can create more fullness in the mid-anterior part of the scalp while still providing broad, natural looking coverage of the frontal area. In the typical Caucasian patient with a density of 2.0 hairs/mm2, follicular dissection will yield approximately:
25% 1 hair implants
50% 2 hair implants
25% 3 hair implants
The 3 hair implants, comprising 25% of the total population, may be concentrated in the central area described above. Alternatively, they could be placed more broadly in a band immediately behind the transition zone of the frontal hairline. In a patient with a density of 2.4 hairs/mm2, the yield would be:
20% 1 hair implants
35% 2 hair implants
30% 3 hair implants
15% 4 hair implants
In this patient, 45% of the implants (30% three hair implants and 15% 4 hair implants) would be available for this purpose. If dissected properly, the 3 and 4 hair follicular units should comfortably fit into the same size sites as the two hair units and should not necessitate any additional trauma to the recipient area for their insertion.
There are obviously an infinite number of permutations when considering all of the qualitative and quantitative characteristics of the patient’s hair. These numbers only serve to illustrate the huge flexibility one has when follicular units are being transplanted to produce natural coverage of relatively large areas in a limited number of sessions. In practice, both pre- and intra-operative judgments are made regarding the forward weighting of the sites and the central concentration of the larger follicular units to produce the most effective results.
Layering is another important element in the aesthetics of the hair restoration process, and this becomes more important as the balding pattern inevitably progresses. The “layering” effect makes hair appear fuller and thicker as one looks deeper into the transplanted area. When implants are weighted, layering serves to accentuate its cosmetic impact. Although both weighting and layering generally require a specific length and styling pattern to be maximally effective, the result is a natural look in normal social settings.
If the goal in a Norwood Class V, VI, or VII patient is to achieve the maximum degree of fullness, and the patient is willing to be committed to styling his hair in a specific pattern, then “side weighting” should be considered (figure 2A). This is accomplished either by placing a greater proportion of the implants on the parted side of the scalp, using larger follicular units on that side, or using a combination of these two techniques. As will be discussed, the larger follicular units must always have a transition zone in front, consisting of smaller units, to look natural.
In situations where there is a great imbalance in the supply/demand ratio, a more exaggerated form of “side weighting” may be appropriate (figure 2B). This might occur in patients with very low density, when open donor harvesting has severely depleted the donor supply, when plugs are scattered in different cosmetic areas (and there is not enough hair to connect them), or when scalp reductions have rendered the patient’s donor supply unharvestable (by severely reducing the donor density and/or laxity). In these situations, we most commonly utilize a variant of side-to-side weighting that we call the “hockey stick.” This takes advantage of dedicated side-to-side grooming and establishes a frame to the face while utilizing a minimal amount of hair. It is accomplished by placing the majority of the implants along the frontal hairline and along the part with some units scattered in areas totally bald. These latter units, which we call “tacking hairs,” serve to anchor the hair combed over it from the more densely transplanted areas. After growth is completed, the patient will have limited styling options, as would be the case whenever hair is not transplanted in a symmetrical, natural pattern.
Aesthetic Nuances: Gradients, Angles, and Swirls
The Transition Zone
The transition zone is the region that leads one’s eye from the totally bald scalp into the thickness of the transplant. It is the most visible part of the reconstruction and therefore the most critical. As in other aspects of the transplant, the key to establishing a natural looking transition zone is to mimic as closely as possible the one that occurs in nature. Fortunately, follicular implants provide us with the tools to accomplish this. Transition zones are seen in the following locations: 1) the frontal hairline, 2) the temples, 3) the balding crown (the posterior transition zone), and 4) the sides (if the forelock becomes isolated). A transition zone is also needed for the integration of transplanted hair into an area of existing hair and to camouflage larger grafts or plugs (beyond the scope of this article).
If one carefully observes a frontal hairline, one does not see a “line,” but a soft feathery zone produced by a gradation of follicular units of increasing size and density. A natural looking hairline can be created by the delicate placement of single hairs, followed by two, three, and possibly four hair follicular units (depending upon the patient’s density). This hair must always be harvested and implanted in the naturally occurring follicular groups for maximum growth and the best cosmetic result.
In women, a “vellus blush” produced by finer hair, is often noted at the frontal hairline. In men, the aesthetic contribution of these vellus hairs is much less significant, if they are present at all. It has been the practice of some transplant surgeons, using more traditional techniques, to harvest donor hair at the nape of the neck in order to capture some of the fine hair that grows in this area. We advise against this practice because the incidence of unacceptable scarring is quite high in this region and the hair in this location may not be permanent. The use of single hair follicular units can generally produce completely natural results, especially in men, where, in contrast to women, thick terminal hairs are commonly seen along the frontal hairline of the mature individual. Follicular units of two and three hairs should not be divided into single hairs as this will increase the risk of poor growth. As discussed, single hair implants should be derived from naturally occurring single hair follicular units. At times, finer populations of terminal hair can be found in areas that are surgically harvestable without placing the patient at unnecessary risk. If this is the case, these may be accessed, although, in our experience we rarely find this necessary. This does not apply to the temples, where the restoration is more problematic in this regard and will be discussed separately.
Another characteristic of the transition zone is that it is extremely irregular and often asymmetric. Since “beauty” in all living things is defined, in part, by their “symmetry” there must be a delicate balance between creating a zone that is “too perfect” and one that does not maximally enhance the patient’s appearance. We find that the random placement of approximately 100 single follicular units in front of a symmetrical band of staggered single units 1 to 3 rows deep will usually achieve the appropriate balance. Behind this, larger follicular units can then be used. It is important to limit the depth of the single hair units, or the zone will appear too thin. If there are extra single hair units produced in the dissection they may be used in other parts of the scalp rather than being all committed to the frontal hairline, or they may be combined together into a single site to increase the fullness of a specific area.
We suggest that sites for single follicular units in the transition zone should be made with a needle that produces an opening no more than 1-1.2 mm. Two, three, and four hair follicular units should be placed in an opening no greater that 1.2-1.5 mm. We feel that larger sites are not necessary, and should be avoided, as they will increase the incidence of dimpling and other scalp deformities. The spacing of sites may be as close as 1.2-1.5 mm with the maximum density of follicular units in the region just behind the transition zone. This will limit visual penetration from the frontal view and create the illusion of greater fullness throughout the scalp, while conserving on the total number of implants needed. In this critical region just behind the transition zone, follicular units should be placed as close together as the mechanics will allow. Great care must be taken, however, to ensure that one site does not “bleed” into the next, as this will create a “slit” which will have less than optimal healing. In other areas, sites should be spaced further apart as discussed in the section entitled Density.
The depth of the transition zone in the frontal hairline should generally be about 1cm at the midline and slightly greater towards the temples. As one extends laterally, the density of site placement should be slightly less, creating a somewhat greater depth of visual penetration. In this location, larger follicular units should be set slightly further back into the hairline to maintain a natural look. These dimensions will of course, vary depending upon the patient’s density, his hair characteristics, and the aesthetics of the individual transplant. People with fine hair, wavy hair or very high density, will look natural with larger groupings placed in a more forward position, and may benefit from having a more compressed transition zone.
Restoring the Mature Hairline
To recreate a hairline that will be appropriate for the transplant patient well into adult life one must understand the progression of the normal hairline with age.2 The adolescent male (those under the age of 16) and most genetically unaffected females, have a frontal hairline which touches the top crease of the brow when the eyebrows are raised (Norwood Class I or “Juvenile” hairline). In other words, hair begins where the action of the frontalis muscle ends, so that growth only occurs on a smooth scalp.
As the male hairline recedes to its mature position, the frontal edge moves backward for a distance of one fingerbreadth (about 1.5 cm) above the brow crease at the midline and approximately 2-4 cm towards the temples. We find that this marking is a more reliable indicator of the “ideal” mature hairline position than the common practice of use of using 4 fingerbreaths above the eyebrow or by dividing the face into “thirds.” The facial proportions of each individual patients will, of course, ultimately determine the aesthetics of the transplant, and all “rules” should serve only as general guidelines. As the corners recede, the frontal hairline forms an acute angle with the temples, differentiating it from the corners of an adolescent or a woman. These changes generally occur between the age of 16-29 and can be gradual or rapid. In the non-balding male, the hairline will be maintained at this point, even as the person ages. This location, therefore, defines the position of the mature male hairline (Norwood Class II) and any migration past this boundary is considered to represent balding.
With some exceptions, the goal should be to recreate a mature hairline. Hair in this position will serve to frame the face and maximize the cosmetic benefit of the transplant. This is especially important at the midline. There is much more flexibility in creating recession towards the temples as hair loss in this region will have much less of an impact on the patient’s overall “look.” Many patients will actually prefer more temple recession, especially those with thin faces, or a family history of a persistent forelock and this variation should also be considered. On the other hand, there is sometimes the temptation to try and conserve donor hair by raising the entire frontal hairline. This will compromise the effectiveness of the transplant and, in our opinion, should be avoided. For most patients, the posterior aspect of the scalp is a much better area than the front in which to conserve hair.
A patient who has been bald for a very long time often resists the suggestion to place the mid-frontal hairline a finger breadth above the brow crease as his memory of hair in this position has long faded. He often points to the top of his head and says that he wants his hair placed further back “so that it won’t be too noticeable.” Our answer is that not only will it not be noticeable in that position but that it may actually make him look worse. Hair added to the top of the head will accentuate frontal baldness. We try to explain that in an aesthetic restoration, one must go back in time to when the patient had hair. One should add the hair to a position where the hair would have been when the patient had it. It often helps the patient if the physician illustrates the difference in appearance between regular balding and the front to back or “A” type balders, who always look worse than their regular Norwood counterparts. This is because the A’s lose the forward position of the frontal hairline and the frame to their face early on, and have marked contrast between the bald scalp and the surrounding hair.
There are a few situations in which the frontal hairline may be placed lower than the mature position or with less temporal recession, but in each case it is important that the patient is clearly informed of the possible long-term consequences. The first situation would be where the patient’s career demands a certain look, such as in acting or modeling. This patient should have a low risk of significant baldness and must be aware that an aggressively low hairline now may compromise his ability to have a balanced, natural look in the future. The second situation would apply to the patient with a very low risk of progressive baldness. An older, stable, Class III patient with no family history of balding, and less than 20% miniaturization in the front part of his scalp would fall into this category. Patients from ethnic origins where the hairlines maintain the adolescent position, such as Asian Indians, will often desire a restoration in this location. This should be considered only if the patient’s density, laxity, and hair characteristics can support this. Women, of course, normally lack bitemporal recession so that a restoration in females should be to the Norwood Class I position. Finally, if one needed to improve the cosmetic appearance of a transplant that was performed improperly (such as one that was to pluggy) and the hairline was already in the proper location, lowering the hairline might be necessary to provide adequate camouflage for unnatural looking grafts, if they were not removed.
There are some situations in which a higher placed hairline is necessary, but as stated earlier, we feel that every attempt should be made to keep at least the mid-portion of the frontal hairline in the forward, mature position. When a patient has very low donor reserves, or will most likely eventuate into a Norwood Class VII, significant bitemporal recession should be built into the transplant from the outset. In general, the more bald one anticipates the crown will become, the more one should recess the temples in order to keep a proper balance. If one simply examines the regular Norwood classification, this balance can be appreciated. The less total volume of hair that a patient has, the less it should be spread around. Trying to cover too large an area with too little hair will leave the patient with a diffusely thin, rather than “patterned” look. The “art” is to strike the right balance between simply achieving “coverage” and producing a pattern that is recognized as being natural.
Another consideration when deciding upon the shape of the frontal hairline, and ultimately the entire transplant design, is forehead width. It is intuitive that for balance, a narrow forehead requires more tapering at the temples and a broad forehead a more broad, rounded hairline. The problem is that the patient with a broad forehead requires a much greater amount of hair to cover the anterior part of the scalp. Since forward weighting is an integral part of the solution to the supply/demand imbalance, a narrow forehead enables the surgeon to concentrate a larger number of implants in a smaller area, whereas the broader forehead does not. However, since in Follicular Transplantation, the implants are already spaced as closed together as mechanically possible in the first procedure, the patient with a wider forehead can actually achieve the appearance of more fullness in this procedure than the patient with a narrow forehead.
The reason for this apparent paradox is related to grooming. With a narrow, more tapered hairline, the first procedure will not give as full a look, but with subsequent procedures, the density can be increased to the point where enough density is achieved for the patient to have a full look with the hair combed straight back. However, if combed side to side , there is not enough breadth for layering to make a significant contribution to the overall appearance. With a broader hairline, more fullness can be achieved with side to side combing after the first session, but the surface area is often too great to achieve sufficient density to produce the same look with straight back combing, even with multiple procedures. In patients with a broad forehead, high density, a loose scalp, and coarse, wavy hair, a full look can also be achieved with the hair combed straight back, but these patients are the exception. If all that can be achieved with a broadly placed hairline is a thin look, this option is, of course, reasonable, as long as this goal is acceptable to the patient in advance of the surgery.
Another option is to try to achieve a higher density in a confined area by recreating a forelock type pattern. This concept is a sound one and has been well described in the article “The Isolated Frontal Forelock. ((Marritt E, Dzubow L. The isolated frontal forelock. Dermatologic Surgery 1995;21523-538.))” However, the approach that these authors use to create this pattern differs. As described by Marritt and Duzbow, the forelock consists of larger grafts surrounded by smaller grafts that are added in stages to soften its appearance. We prefer to transplant the entire forelock in one session using Follicular Transplantation and then add fullness in subsequent sessions, rather than to need these sessions to make the original transplant look more natural. In other words, to avoid the “process plugginess,” that Marritt describes, which, in our opinion, rarely goes away. With follicular implants, the first procedure, although possibly too thin, will stand on its own. In addition, subsequent procedures will be hidden within the boundaries of the first; there will be not any scarring or surface deformity around the larger grafts, and it will be totally undetectable as a transplant, even when the hair is wet or not combed “just so.”
We feel that establishing the frontal hairline is the single most important function of the first procedure. Once the hairline is restored to its proper position, the second procedure can be used to further refine it. The most common “refinement” is to increase its density. As was discussed in the section on Density, there are mechanical limitations to the density that can be achieved in a single procedure. This is in part due to the bulk of the follicular unit itself and the physical restrictions on how close together the sites can be made. With a subsequent session, the spacing can be as close as in the original procedure, essentially doubling the density of the first. This is possible because the small follicular implants of the second procedure contain little bulk and will easily fit between the implants of the first, once complete healing has occurred (figure 3).
Another refinement of the frontal hairline is increasing the irregularity of the transition zone. The random placement of hair at the frontal edge is always part of the first procedure, however, it is impossible to exactly predict the aesthetic impact until the hair actually grows in, given the infinite combination of hair characteristics. It is much less common that a second procedure would be used to make the hairline more uniform, as irregularity is one of the defining characteristics of a natural looking hairline.
On rare occasions, the frontal hairline is either lowered or flattened (the corners blunted) in the second procedure. If the hairline is placed properly in the first session, this should not be necessary, but at times, after the patient has seen the first transplant fully grown in he wants a more “youthful” look. We consider this option only after reviewing the long-term aesthetic consequences with the patient, and only when the patient’s donor supply and hair characteristics are optimal, and there is little risk for him to be extensively bald. The vast majority of the time, when patients complain that their hairline is placed too high, it is because they are looking too far into their transition zone. Simply doubling up on the density without changing the position of the hairline will often solve the problem.
One of the most dramatic and interesting types of frontal hairline patterns is the “widow’s peak.” The widow’s peak is not simply a triangular dip at the midline but a series of deviations from the normal hairline. For this reason, we generally do not recommend reproducing widow’s peaks, but suggest reconstructing the hairline according to the way that is most natural for the vast majority of the population. In this way specific attention is not drawn to the hairline. For patient’s that do desire a “peak,” the following should be considered: 1) the peak is often associated with a bi-concave rather than convex hairline, 2) it is often asymmetrical, and this asymmetry can be due to the shape, the apex being off center, or having one side concave and the other convex, 3) the hair often points to one side rather than forward, and 4) two procedures are generally required for the restoration.
Just as great care must be directed toward creating the frontal hairline, other parts of the restoration may be directly visible, or become visible over time. In a patient with a limited supply of donor hair, or in patients who continue to bald extensively, but who choose not to have further procedures, the transplanted top part of the scalp will gradually become dissociated from the sides. Fortunately, since this pattern occurs in nature, it is cosmetically acceptable (although less than ideal). To plan for this eventuality, a transition zone must be built into the lateral aspects of the transplant in a way that is analogous to the frontal hairline, even if it is not exposed at the time the transplant is performed. Single hair follicular units that were not needed in the front (in order to produce a fuller look) should be put aside for this purpose. If the sides recede there will be a soft lateral border that will look natural and “stand on its own.” As will be discussed in the section Reconstructing the Crown, the posterior aspect of the top or vertex must be treated in a similar fashion.
Hair Direction
It would seem the statement “hair should be placed into the scalp at an angle in which it originally grew” is so obvious that it need not be stated in a professional journal on hair transplantation. However, we find that the single most common error in judgment that hair transplant surgeons make is to place the hair either perpendicular to the scalp or in the direction that the patient plans to groom his hair. In the first case, the hair will be ungroomable and, regardless of the size of the implants, will always look unnatural. In the second case, the hair will tend to lie flat and lack the normal “bowing” that gives the hair its full appearance when combed or styled away from the direction that it naturally grows. The direction of hair often reveals the right or left “handedness” of the inattentive transplant surgeon who orients the hair in the proper forward direction on the side of the patient that he is standing on, but places it more perpendicular to the surface as he reaches across to the other side of the patient. The frequent repositioning of the patient and/or surgeon while creating the sites can easily avoid this problem.
We feel the single most useful clue to the appropriate way to angle the recipient site is to observe the patient’s existing hair. Even in very bald areas there are usually a few vestiges that will indicate the orientation of the original terminal hair. When this information is not available due to extensive balding, a few simple rules can be followed: 1) hair anterior to the crown (from the vertex forward) points slightly forward, with the angle becoming more acute until it reaches the anterior hairline where it is essentially horizontal to the ground (regardless of the slope of the forehead) and 2) the direction of hair in the frontal hairline always points forward, rather than radially, and only deviates significantly from this as one approaches the temples (figure 4).
Occasionally, a transplant is performed in a patient with a persistent frontal swirl or cowlick. As with the “widow’s peak,” we generally disregard this pattern in order to reconstruct the hairline according to the way that is most natural for the vast majority of the population. This conservative approach is appropriate since the “lick” will generally disappear over time. In addition, the frontal cowlick is usually partly composed of fine vellus hair which produces a look that is so difficult to copy exactly (the swirl in the crown is different in that it is formed from terminal hairs). If the patient desires to restore his frontal cowlick, as might be the case if it was an identifying family trait, it should be performed only in patients who are not likely to be extensively bald. At least two procedures, consisting of exclusively single hair follicular units, would be required for the reconstruction.
Temple Restoration
Temple hairline restoration should be undertaken only with great caution and in carefully selected patients. Often, after the frontal restoration is complete, receded temples are no longer bothersome to the patient. For this reason, we generally advise patients to complete the frontal restoration before even considering the temples. Temple restoration may be considered when the sides have receded to such an extent that they no longer look balanced after the front and top have been restored or if there is great asymmetry between the two sides. For women with androgenetic alopecia who are candidates for a transplant, temporal restoration can be used to restore the shape of the “female” frontal hairline. Permanent hair loss in the temples after face lifts can also be restored . We have occasionally performed temple reconstruction in male patients that have had sex change operations or face lifts. The nuances of temple restoration are also important when treating patients with traction alopecia, alopecia marginalis, and various forms of stable scarring alopecia involving this region of the scalp.
There are a number of problems intrinsic to temporal restoration. The major one, which has been mentioned previously, is that in men with androgenetic alopecia, significant temporal recession often portends an extensive balding pattern. Thus, the very patient who may need temple restoration the most is the one at greatest risk to having an unnatural, unbalanced look after it is complete. For this reason, restoring the temples should be reserved for those patients who have an excellent donor supply and who will not likely progress past a Norwood Class VI, even on the long term. Often the temples will continue to recede, requiring further surgery, and demanding a greater proportion of the limited donor supply. This problem can be exacerbated if the surgery causes further acceleration of the hair loss behind the transplanted area.
Another problem is that, unlike the frontal hairline in men, the temples are always composed of fine, vellus hairs at the frontal edge, and there is not a consistently reliable donor source for these hairs. In the majority of patients, the thick terminal hairs harvested from the mid-portion of the permanent zone are not a good match for the finer temple hair, but on occasion the match is close enough to make the procedure practical. If a change in hair characteristics should occur (an infrequent side effect of hair transplantation), then the resultant “wiry” hair may look unnatural.
Following the normal hair direction at the temples is probably the most difficult aspect. As always, before any restoration is attempted, it is important to observe the temples of many normal individuals. Hair at the most lateral aspect of the frontal hairline points forward. In the transition to the temples, the hair abruptly changes to a diagonally forward and downward direction, and then at the apex of the temple it abruptly changes to a backwards and downward direction. The angle that the hair exits from the skin is extremely acute so that the instrument creating the sites must be placed almost flat along the surface of the skin.
The transition zone of the temples contains a much greater depth of one and two hair follicular units compared to the frontal hairline. This, of course, must be reduplicated in order to keep the fine, delicate appearance. The depth of the single hair units alone can often exceed 1 cm. In addition, very small recipient sites (~1 mm) must always be used to prevent skin surface deformity. Temple hair transplants will often fail to grow if the depth of the hole is not precisely made or if the implants are traumatized during insertion. Placing grafts into such small, angled openings is extremely difficult and requires significant experience on the part of both doctor and staff. Despite these problems and the special skills required, temple restorations can be successful in very select patients.
Reconstructing The Vertex and Crown
When to treat the crown is an extremely important issue in both the short and long-term planning of the transplant. Its indications are discussed elsewhere (see Follicular Transplantation: Patient Evaluation and Surgical Planning in this publication) and are beyond the scope of this article.
Although the terms “vertex” and “crown” are often used interchangeably, they are distinctly different regions of the scalp, each with unique characteristics and requiring different approaches to the restoration. They are shown in figure 1A and are defined as follows. ((Salasche SJ, Bernstein G, Senkarik M. Surgical Anatomy of the Skin, Connecticut: Appleton & Lange, 1988:152.)) Vertex – the back part of the top of the scalp anterior to the crown, where the hair points in a forward direction. It is the highest point of the scalp. Crown – the convex area where the occipital and parietal areas join, and the hair takes on a swirling pattern.
Regardless of the patient’s Norwood classification, if there is sufficient donor hair, the transplant should always extend far enough backward to cover all of the bald scalp up to, and including, the vertex. Since there are no boundaries or lines of demarcation between the front, top and vertex, these regions should be treated as a single cosmetic unit. The vertex is a natural stopping point for the transplant for a number of reasons: 1) it is clearly distinguishable from the crown by the directional change of the hair and by the curvature of the skull, 2) it defines an area that is limited enough in size to be completely covered in most patients, 3) its posterior boundary is semi-circular, so that further balding posteriorly maintains a natural shape to the bald crown if it is left untransplanted, 4) the transplanted hair can be combed back to cover the crown, 5) the pattern that results when the transplant extends through the vertex is commonly seen in nature, and 6) the naturalness of the distribution will be unaffected by further balding (i.e. expansion of the crown).
Transplanting through the vertex is accomplished simply by extending the transplant backward to the natural arc that defines the area, and then by creating a posterior transition zone (posterior hairline). This is accomplished in the same manner as the transition zone at the frontal hairline, except in reverse. There is the same progression of one, two, and three hair follicular units, and the random distribution of single hair units at the leading edge. The major difference is that the transition zone tends to be somewhat wider. If possible, the posterior transition zone should extend through (over the top of) the vertex so that the hair will drape naturally over the crown and give the head a more rounded shape when viewed from the side. It is also important to remember that when the surgeon anticipates that the transplant will stop at the vertex, and not extend into the crown, the temples should be slightly more receded for optimum balance.
When treating the crown, one must recognize that the normal crown has a delicate swirl of hair at its center with progressively increasing areas of density as one extends outward. This area is essentially a transition zone with small follicular units at the very center and with hairs exiting the scalp at very acute angles. As a rule, the swirl is off center rather than midline and can, on occasion, be multiple.
The delicate nature of the normal crown explains why the placement of anything but the very smallest implants in its center will produce an unacceptable appearance, and the use of larger minigrafts or plugs in this area, especially when improperly oriented, can be a cosmetic nightmare for the patient. The natural, acute angle of emerging hair cannot be easily duplicated with the larger grafts, and most importantly, the density of the larger grafts can never be maintained as the balding progresses. Placing a few larger grafts in the center of a young person’s crown to mask the early stages of balding is using poor judgment as is placing them in the areas of earliest temple recession in a young patient who may become extensively bald. Both seemingly simple and innocuous procedures commit the patient to a lifelong series of poorly planned hair transplant surgeries.
The key to transplanting the crown is to recreate a tight swirl of follicular units, in exactly its original angle, location and pattern. A fine surgical marking pen should be used to reproduce this pattern prior to making the sites. We find it easiest to create sites in a small number of thin, outward spirals, that set the pattern for the remainder of the sites, rather than to fill in discrete areas at one time. The best cosmetic results will be obtained if the larger follicular units are used anteriorly and the smaller ones inferiorly. It is important that the hair in the anterior crown extends into, and integrates with the vertex hair without any abrupt directional changes, and is transplanted in a broad enough fashion to meet the entire circumference of the vertex.
Because of the radial expansion of the crown, any significant increase in size will require further surgery. This is why it is so important to be conservative when deciding to transplant the crown and to make certain that there are always enough donor reserves to anticipate a worst case scenario, especially in the younger patient when his future balding is so unpredictable. One should always remember that hair committed to the crown will not be available for the front (which is cosmetically more important). This supply/demand problem is intrinsic to all hair restoration surgery and is, in our opinion, not solved by such procedures as scalp reductions and scalp lifts. ((Bernstein RM. Are scalp reductions still indicated? Hair Transplant Forum Int
1996; Vol 6 No 3:12-13.)) Totally avoiding the crown in situations of extensive balding is better than a failed attempt at coverage, which could leave the patient with a lifelong cosmetic deformity.
When crown coverage is accomplished by creating a tight, but delicate swirl of follicular units spiraling outward in the appropriately selected patient, the transplanted area can provide for natural, permanent, umbrella-like coverage if the bald area expands, minimizing the need for further surgery and committing only a conservative amount of hair to this area. If expansion does occur, relatively less hair may be needed to follow the balding radially.
If coverage of the crown is not possible due to a limited donor supply, then single follicular unit “tacking hairs” may be lightly scattered over this area to provide an anchoring for the vertex hair which can then be combed back over it. With proper grooming, this small amount of hair can anchor the longer hair from the surrounding areas in a way that it will be less affected by wind or rain. Since the spacing between these tacking hairs is so great, their use could be continued if the balding were to progress, without requiring too much hair, and since they contain only one hair each, they have little cosmetic value and would not present a problem if the hair in the posterior scalp were kept very short.
Racial Variations
Before concluding our discussion, we would like to briefly point out some important racial differences that that can affect the outcome of the transplant. In measuring densities in over 5,000 patients, we have observed the average donor area to have approximately 1 follicular unit/mm2. Although the donor densities of our balding patients may not be representative of the general population, this number is extremely helpful in making clinical judgments with regard to our surgery. It is interesting that similar density measurements were obtained histologically by Headington. ((Headington JT: Transverse microscopic anatomy of the human scalp. Arch Dermatol 1984;120:449-456. )) In addition, we find that each follicular unit contains, on the average, 2 hairs, yielding a density of 2 hairs/mm2.
These numbers, however, actually refers to the average Caucasian patient. We find that follicular characteristics, in fact, vary significantly between the different races. The following table compares some easily measurable aspects of the follicular unit in three different races.
The genetic differences in the follicular unit may have adaptive value. It is possible that in Africans, the low density in high follicular groups with darkly pigmented hair enhances photoprotection and minimizes heating of the skin. The curly hair, in tight groups of three, may act like a scaffolding that holds the hair off the surface of the scalp (to cool it) and in a tight meshwork (that blocks the sun). The following video-scans illustrate typical Asian and African scalps (figure 5).
We transplant Asian hair in much the same manner as Caucasian hair, except that in Asians with coarse, straight hair and light skin, it is critical to use a larger percentage of single hair follicular units in the transition zone. Because of the heavy weight of each individual hair, more “bulk” may be achieved in the front part of the scalp, but placing too many units in the anterior portion may limit coverage in other areas, due to the inherently low donor density.
With African hair, modifications must be made in the dissection of the implants in order not to damage the follicular units, which tend to be larger and curved. Slightly larger recipient sites must be created to accommodate the larger implants, and they must be spaced further apart. The very low follicular density would appear to severely limit the success of the transplant, but in fact, the three haired units produce “kinky” hair that more than compensates for the low numbers of groups, and enables patients with this hair type to achieve among the best cosmetic results.
Skin and hair color contrast among the different races also greatly impacts the surgery. For persons of Scandinavian descent, with blonde hair and light skin color, the illusion of more fullness may be achieved even though the hair might be very fine in diameter. The fine diameter hair also permits larger follicular units to be placed further forward in the transition zone. An “Afro” hair style on a black haired person with very dark skin will give the appearance of greater fullness, as the dark skin color fills in any gaps between the hair. This is in contrast to an Asian’s black, straight hair which often overlies light skin and appears less dense due to the light color showing through.
Hairline design should also be tailored to the specific racial backgrounds of the patient. In certain families of southern Asia and those of Middle Eastern descent, the hairline tends to be flatter than the hairline of Northern European individuals. These patients often bald in a diffuse pattern, with a juvenile hairline that persists well into middle age. This poses significant problems in selecting a restoration plan which meets both the short and long-term goals of the patient. There are so many other racial and ethnic elements that affect the aesthetics of coverage, the surgeon should have great familiarity with the normal hair patterns and characteristics specific to each group before attempting the transplant.
Conclusion
This article has focused on a number of important “aesthetic judgments” that should be made to ensure the best cosmetic result when performing Follicular Transplantation. We feel that in hair restoration surgery the physician’s goal should always be directed toward finding ways to most accurately mimic nature. The more one’s own interpretation deviates from the template set by nature, the less natural the results will be. It is hoped by these authors that as a result of this writing, many of the “aesthetic judgments” described above will be viewed as logical solutions to the supply/demand dilemma that all of us face when trying to restore a person’s hair.
The following figures show a case study that illustrates a number of the techniques that have been discussed.
 Figure 6. Preoperative full face view of a Norwood Class Va/VI 38 y/o male with medium fine, light brown/blonde hair. The patient had a slightly below average donor density which varied from 1.9 hairs/mm2 at the midline to 1.5 hairs/mm2 on the sides.
Figure 6. Preoperative full face view of a Norwood Class Va/VI 38 y/o male with medium fine, light brown/blonde hair. The patient had a slightly below average donor density which varied from 1.9 hairs/mm2 at the midline to 1.5 hairs/mm2 on the sides.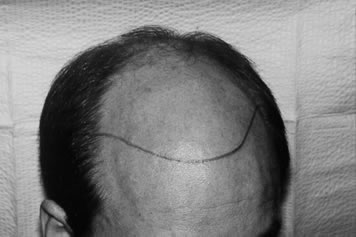 Figure 7. Pre-op with hairline drawn 1.5 cm above the upper brow crease at the midline.
Figure 7. Pre-op with hairline drawn 1.5 cm above the upper brow crease at the midline.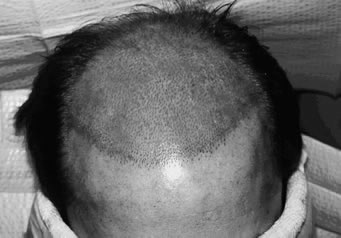 Figure 8. Photo taken immediately after the creation of 2,500 recipient sites. Note the feathered transition zone. The sites measured 1.1 mm along the frontal hairline and 1.5 mm in the remainder of the scalp.
Figure 8. Photo taken immediately after the creation of 2,500 recipient sites. Note the feathered transition zone. The sites measured 1.1 mm along the frontal hairline and 1.5 mm in the remainder of the scalp. Figure 9. Photo taken immediately after the insertion of 2,500 follicular implants consisting of 1072 single-hair units, 1142 two-hair units, and 286 three-hair units. As to be expected in a patient with below average density, there were no four hair follicular units harvested.
Figure 9. Photo taken immediately after the insertion of 2,500 follicular implants consisting of 1072 single-hair units, 1142 two-hair units, and 286 three-hair units. As to be expected in a patient with below average density, there were no four hair follicular units harvested. Figure 10. Top view showing marked forward weighting of recipient sites. There was also central concentration of the larger follicular implants.
Figure 10. Top view showing marked forward weighting of recipient sites. There was also central concentration of the larger follicular implants.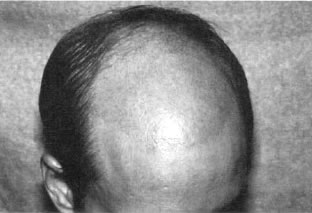 Figure 11. Seventeen days post-op with most of the transplanted hairs shed and faint erythema on an otherwise normal, non-scarred scalp.
Figure 11. Seventeen days post-op with most of the transplanted hairs shed and faint erythema on an otherwise normal, non-scarred scalp. Figure 12. Frontal view 4 months post-op showing early light, but natural, coverage.
Figure 12. Frontal view 4 months post-op showing early light, but natural, coverage. Figure 13. Top view at 5 months post-op. The hair is too short to have any significant layering.
Figure 13. Top view at 5 months post-op. The hair is too short to have any significant layering. Figure 14. Top view with the hair longer so that some layering can be achieved with left to right grooming (6½ months post-op, second procedure).
Figure 14. Top view with the hair longer so that some layering can be achieved with left to right grooming (6½ months post-op, second procedure). Figure 15. Close-up of the frontal hairline at 11 months showing a natural transition zone and layering.
Figure 15. Close-up of the frontal hairline at 11 months showing a natural transition zone and layering. Figure 16. Full face view 11 months post-op showing dramatic change in appearance after a single procedure.
Figure 16. Full face view 11 months post-op showing dramatic change in appearance after a single procedure. Figure 17. Close-up view 6½ months after a second procedure of 1186 follicular implants. The second procedure was performed 11 months after the first. Note that compared to the first session, where the transplanted hair has fully “matured” and is silky in appearance, the hair in the second session (only 6½ months post-op) is slightly more wiry. This will correct over the next
Figure 17. Close-up view 6½ months after a second procedure of 1186 follicular implants. The second procedure was performed 11 months after the first. Note that compared to the first session, where the transplanted hair has fully “matured” and is silky in appearance, the hair in the second session (only 6½ months post-op) is slightly more wiry. This will correct over the nextseveral months.
 Figure 18. Full face view showing the increased density achieved with the second procedure. The second procedure was also performed with forward weighting. In this procedure, 440 single-hair units, 575 two-hair units, 170 three-hair units, and one four-hair unit were implanted. At the time this photo was taken, the patient was 6½ months post-op so that the full cosmetic impact of the second procedure is not appreciated.
Figure 18. Full face view showing the increased density achieved with the second procedure. The second procedure was also performed with forward weighting. In this procedure, 440 single-hair units, 575 two-hair units, 170 three-hair units, and one four-hair unit were implanted. At the time this photo was taken, the patient was 6½ months post-op so that the full cosmetic impact of the second procedure is not appreciated.


