
Robert M. Bernstein, M.D.
Hair Transplant Forum Intl. 2013; 23(3): 91-92.
For years we have debated the pros and cons of follicular unit transplantation (FUT) and follicular unit extraction (FUE). A person’s age and the ability to assess the permanence of the donor area are critical variables in determining which patients are good candidates for surgery. This paper discusses FUT and FUE from the vantage point of these variables.
The effects of FUE and FUT on the donor zone are not so straightforward. Both procedures alter this region of the scalp, but in different ways and with different consequences. In FUE, the donor zone is thinned by directly removing follicular units. The harvesting leaves hundreds to thousands of tiny, white, round scars. In FUT via strip harvesting, the donor zone is thinned as the scalp is stretched during the closure. The result is a single, long (hopefully thin) scar. A concern with both is that, as baldness progresses and/or as hair quality changes, the scars may become visible over time.
With FUT, if the hair is kept very short, the scar will be immediately visible, but if it is kept long, then even over time the scar should be easily camouflaged with hair. This is, of course, providing that the incision is properly placed in the midpoint of the permanent donor area and the scar is not excessively wide.
In contrast, the advantage of FUE is that the hair can be worn fairly short. This is its great appeal, particularly in younger patients. However, since the area of harvesting is generally five times the area of a donor strip for the equivalent number of grafts, this necessitates a donor area five times as wide (i.e., 5x as high if the length is maximized in both). Unfortunately, this may not bode well for the patient if the safe donor area turns out to be smaller than one had anticipated.
If a person evolves into a Norwood VII, with a thin donor zone, then the scarring of FUE—although quite inconspicuous when the person had hair—will become visible over the top of the fringe. An additional problem, of course, is that the transplanted hair that was harvested from this area will disappear.
If a person’s donor hair thins significantly, then any scarring (whether it is the linear scar of FUT or the small, round scars of FUE) may become visible. Therefore, in either procedure, having a relative degree of confidence in your assessment of the ultimate fate of the donor zone is critical to the planning of the surgery. The problem is that it is very difficult, if not impossible, to identify the safe, permanent donor zone when a person is young. In fact, at a young age, it is not always possible to determine with certainty if ANY of one’s hair will be permanent or what the ultimate quality of that hair will be.
The simple solution is to not operate on younger patients regardless of the technique. But what constitutes a “younger” patient? As a general rule, when treating androgenetic alopecia, I consider 25 to be the (somewhat arbitrary) minimum age for hair transplant surgery. Before this age, densitometry used to measure miniaturization is quite unreliable and, therefore, the degree of ultimate balding is very hard to predict.
Patients who bald at a very young age are prone to develop more extensive hair loss than those who thin later in life. Therefore, their donor supply may not be sufficient for a cosmetically successful hair transplant. For example, if a person is to eventuate into an advanced Norwood Class VI or VII, there often is not sufficient donor hair for adequate crown coverage. Restoring a mature hairline, adding hair to the mid-scalp and providing some light coverage to the crown, would be perfectly acceptable for a 40- or 50-year-old. However, the 20-year-old with an incomplete hair transplant and a still balding crown might, in retrospect, have preferred to have just shaved his head. After surgery, this option would be gone.
It is important to stress that the earlier hair loss begins, the more extensive it is likely to become. In so many cases, medication, rather than surgery, is the best initial choice for younger patients. It gives them time to think about their options and to adjust to the fact that, regardless of surgery, they will not have a full head of hair or the low hairline that they once had. It also gives them the opportunity to seek the opinion of family and friends. In all cases involving younger patients, the decision to have surgery should be well thought out and never done in haste.
Case Study
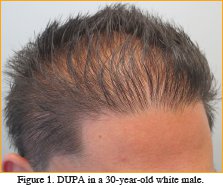
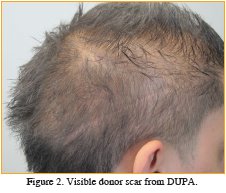
Patient JB is a 30-year-old male complaining of progressive hair loss and a visible donor scar. He had two hair transplant procedures at age 21 and 22. At the time, he was told he was a good candidate for surgery. Densitometry was not performed. After the procedure, the patient used finasteride and minoxidil. In spite of a hair transplant and medical therapy, the patient’s hair continued to thin. Within a few years, his donor scar became obvious, presenting a cosmetic problem far greater than his hair loss.
On physical examination, JB had a persistent frontal hairline, generalized thinning, and a readily visibly donor scar. Densitometry revealed a donor density of 1.2 follicular units/mm2 and 90% donor miniaturization consistent with a diagnosis of diffuse unpatterned alopecia (DUPA). ((Norwood, OT. Male pattern baldness: classification and incidence. So Med J. 1975; 68:1359-1365.)) (See Figures 1 and 2.)
Surgical options for this patient remain limited, as there is no permanent zone to harvest hair (with the idea of using FUE and placing hair into the scar). Surgical re-excision will not eliminate the scar. Scalp Micro-pigmentation (SMP) was discussed, but will give only a partial cosmetic improvement.
Discussion
This is a case of a surgeon operating on a patient that was too young and failing to diagnose DUPA. DUPA is a contraindication for hair transplantation. ((Bernstein, R.M., and W.R. Rassman. Follicular transplantation: patient evaluation and surgical planning. Dermatol Surg. 1997; 23:771-784.)) The instability of the donor area in DUPA renders both FUT and FUE ineffective hair restoration procedures.
Classic DUPA, presenting as rapidly progressive, generalized thinning at a young age, is just one end of a spectrum of diffuse thinning that eventuates in the loss of one’s donor zone. Not uncommonly, one can observe a similar, albeit less aggressive process occurring a little later in life—a condition this author refers to as “Adult DUPA.” The important point is that, regardless of the name, the long-term stability of the donor area is often difficult to ascertain and always becomes easier with time.
The appropriate management of this patient would have been to postpone any consideration of surgery to a later date. Although it is difficult to specify exactly at what age surgery might be considered, it is certain that with time a diagnosis of DUPA, or any of its variants, would become more obvious, both with densitometry and to the naked eye. A proper diagnosis would have spared this young man a failed hair transplant procedure and an unsightly donor scar.



