
Robert M. Bernstein, M.D., William R. Rassman
Hair Transplant Forum International 2007; 17(2): 41, 49-51.
In evaluating a person with androgenetic alopecia for a hair transplant, typically the physician determines the patient’s Norwood Class, designs a hair line, delineates the extent of coverage, “eyeballs” the donor area, and then decides upon the appropriate number of grafts. Taking specific measurements of hair density and donor miniaturization are not routinely performed. However, donor density and miniaturization are important variables in deciding which patients are good candidates for hair transplantation and are useful in determining how many grafts are needed in the procedure.
Densitometry is a technique that analyzes the scalp under high-power magnification to give information on hair density, follicular unit composition and degree of miniaturization. It can be used to help evaluate a patient’s candidacy for hair transplantation and help predict future hair loss. More recently, video-microscopes have been developed that can project the image onto a computer screen and provide a permanent digital record. This paper describes the value of taking objective measurements, using densitometry or video-microscopy, in the hair transplant evaluation.
Background
One of the earliest methods of measuring hair density was devised by Bouhanna, who used camera attachments to create a “phototrichogram,” an ultra close-up photograph of hair exiting the scalp. This method provided the capability to document the quality and quantity of hair shafts. However, the disadvantage of this innovation was that an assessment could not be done until after the film had been developed. ((Bouhanna P: Phototrichogram: a technique for the objective evaluation of the diagnosis and course of diffuse alopecia. In W Montagna et al. (eds). Hair and Aesthetic Medicine. Roma, Salus Ed. 1983: 277-280.))
In 1993, Rassman introduced a small hand-held instrument, the Hair Densitometer, to make densitometry easy to perform during a consultation. ((Rassman WR, Pomerantz, MA. The art and science of minigrafting. Int J Aesthet Rest Surg 1993; 1:27-36.)), ((Rassman WR, Carson S. Micrografting in extensive quantities; The ideal hair restoration procedure. Dermatol Surg 1995; 21:306-311.)) The hair densitometer is a self-contained, portable, device that houses a magnifying lens and an opening of predetermined size. [Figure 1] The hair is clipped short (~ 1mm) and the unit is placed directly on the scalp. An assessment is made from a standard 10mm2 field. Multiple measurements taken from different parts of the scalp are often helpful, particularly if there is significant variability from one location to another. ((Bernstein RM, Rassman WR, Seager D, Shapiro R, et al. Standardizing the classification and description of follicular unit transplantation and mini-micrografting techniques. Dermatol Surg 1998; 24: 957-63.)) An advantage of the hand-held densitometer is that it is inexpensive and readily available to be used during the consultation and can provide immediate information regarding a patient’s candidacy for surgery.

Figure 1. The Rassman Hair Densitometer

Figure 2. Micro-VID Digital Hand Held Microscope
A number of other hand-held instruments to measure density have been developed with the similar basic elements of magnification, illumination and a calibrated field or ruler. With more recent technology, digital trichograms allow the physician to take quantative measurements of hair shaft diameters and provide an immediate, permanent record of this information. ((Stough DB, Haber RS. Hair Replacement: Surgical and Medical. St. Louis: Mosby-Year Book, Inc., 1996: 139-140.)), ((Van Neste D, Dumortier M, De Coster W: Phototrichogram analysis: technical aspects and problems in relation to automated quantitative evaluation of hair growth by computer assisted image analysis. In Van Neste D, Lachapelle JM, Antoine JL (eds). Trends in Human Hair Growth and Alopecia Research. Dordrecht, Kluwer Acad. Pub, 1989: 155-165.)), ((Hayashi S, Hiyamoto I, Takeda K: Measurement of human hair growth by optical microscopy and image analysis. Br J Dermatol 1991; 125:123-129.)) [Figure 2]
The densitometer was initially used to quantify a patient’s donor density, to estimate the total number of grafts that could be safely obtained from the donor area, and help predict the change in reserves over subsequent transplant sessions.3 With the introduction of Follicular Unit Transplantation in 1995, these authors began to use densitometry to assess follicular unit composition (the number of terminal and miniaturized hairs that each individual unit contained) and follicular unit density (the spacing between units), as these additional factors were found to be important in the assessment of the donor supply and in the overall surgical planning of follicular unit transplantation procedures. ((Bernstein RM , Rassman WR, Szaniawski W, Halperin A: Follicular Transplantation. Intl J Aesthetic Restorative Surgery 1995; 3: 119-32.)), ((Bernstein RM, Rassman WR: The logic of follicular unit transplantation. Dermatologic Clinics 1999; 17 (2): 277-95.)), ((Bernstein RM, Rassman WR: Follicular Transplantation: Patient Evaluation and Surgical Planning. Dermatol Surg 1997; 23: 771-84.)) The use of densitometry was soon expanded to guide the surgical treatment of those with racially distinct hair characteristics, to improve the diagnosis and treatment of balding women, and to further define the conditions of diffuse patterned and unpatterned hair loss.10, ((Bernstein RM, Rassman WR: The Aesthetics of Follicular Transplantation. Dermatol Surg 1997; 23: 785-99.)), ((Norwood OT. Male pattern baldness: classification and incidence. So. Med. J 1975; 68:1359-1365.))
A number of other hand-held instruments to measure density have been developed with the similar basic elements of magnification, illumination and a calibrated field or ruler. With more recent technology, digital trichograms allow the physician to take quantative measurements of hair shaft diameters and provide an immediate, permanent record of this information.5-7 [Figure 2]
The densitometer was initially used to quantify a patient’s donor density, to estimate the total number of grafts that could be safely obtained from the donor area, and help predict the change in reserves over subsequent transplant sessions.3 With the introduction of Follicular Unit Transplantation in 1995, these authors began to use densitometry to assess follicular unit composition (the number of terminal and miniaturized hairs that each individual unit contained) and follicular unit density (the spacing between units), as these additional factors were found to be important in the assessment of the donor supply and in the overall surgical planning of follicular unit transplantation procedures.8-10 The use of densitometry was soon expanded to guide the surgical treatment of those with racially distinct hair characteristics, to improve the diagnosis and treatment of balding women, and to further define the conditions of diffuse patterned and unpatterned hair loss.10-12
Miniaturization
Normally, follicular units contain 1-4 terminal hairs of uniform diameter and, occasionally, fine vellous hairs, with the two hair populations being clinically distinct. In androgenetic hair loss, the action of DHT causes individual terminal hairs in some follicular units to miniaturize, where they begin to decrease in diameter and in length until they resemble vellous hairs. Eventually, these hairs will disappear. In androgenetic alopecia, hairs in varying stages of involution (and thus of varying diameters) cause these two distinct populations of hairs to merge into one continuum. The changes eventually cause visible thinning in affected areas, but may initially be detectable only through densitometry.
At first, miniaturization involves only one or two hairs in select follicular units, but eventually progresses to involve all the hair follicles in genetically susceptible areas. It has been the observation of these authors that a shift from focal to generalized miniaturization precedes the actual loss of affected hairs, so that total hair counts remain relatively constant until end-stage baldness.8 Said another way, the progressive thinning associated with androgenetic hair loss (particularly in the early stages) is caused by a decrease in the hair shaft diameter of an increasingly larger number of hairs, rather than by the actual loss of individual hair follicles. [Figures 3 and 4.]
Miniaturization, unfortunately, can also occur in the back and sides of the scalp. When it affects a person’s donor area, it will have profound implications for surgery. Although miniaturization in the donor area is a relatively uncommon occurrence in men, it is quite common in women, explaining why so many more men with hair loss are candidates for surgery compared to women. In all cases, donor miniaturization must be assessed prior to considering surgery.
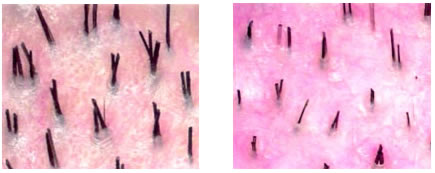
Figure 3 (left image): Follicular units containing normal, full thickness hair.
Figure 4 (right image): Follicular units containing miniaturized hair
Densitometry Measurements
Densitometry is extremely helpful in evaluating patients for hair transplantation. When determining which persons are candidates for hair transplantation, it can be used to measure the absolute donor hair density (i.e. # of hairs/mm2), the composition of follicular units (i.e. the number of 1-, 2-, 3- and 4-hair units), and the degree of miniaturization.
Although the precise hair density and composition of follicular units will not be known until after the donor strip has been completely dissected, at the time of the consultation, densitometry can tell the doctor the approximate hair density. This will enable him to determine how much hair will be obtained from a certain size strip or how large a strip will be needed for a required number of follicular unit grafts.
Densitometry will also give information regarding the cosmetic impact of the hair restoration. Other hair characteristics being equal, if a person has a high number of 3- and 4-hair grafts, he/she would be expected to have a fuller hair transplant than a person with predominately 1- and 2-hair follicular units.
For example, a typical Caucasian would have follicular units in his/her donor area that contained, on average, 2.25 hairs each. If there were 1 follicular unit per mm2 in the donor area (0.9 to 1.0 is normal) then one would need 2,500mm2 of donor tissue for a 2,500 graft procedure. A donor strip that was 1cm wide would need to be approximately 25cm long to contain 2,500 follicular unit grafts. See the following table.
Figure 5. Follicular Unit composition in a typical hair transplant.
Stereo-microscopic dissection of the donor strip would yield approximately 14% 1-hair grafts, 53% 2-hair grafts and 33% 3- and 4-hair grafts. The single-hair grafts would be used to create a soft, natural frontal hairline and the 3- and 4-hair grafts would be used in the forelock area to create the appearance of central density.
Small variations in follicular unit density can have a significant impact on the procedure. A person of similar hair shaft characteristics (i.e. hair diameter, color and wave) that had 2.0 hairs per follicular unit, also spaced 1mm apart, would require exactly the same size strip for a 2,500 graft procedure. In this case, however, the follicular units would, on average, have less cosmetic value and the person should expect a thinner look from the surgery as only 17% of the grafts contain 3- or 4- hairs. In addition, the ability to create central density via graft sorting would be reduced. On the other hand, with a donor density of 2.4 hairs per unit, 40% of the grafts will contain 3- or 4-hairs and the ability of the surgeon to create density in the forelock area using only naturally occurring follicular unit will be significant (Figure 6.)
Figure 6. The distribution of follicular units in 2,500 graft hair transplants of varying donor densities.
If we look at the total number of hairs contained in the follicular units, we note that for a 2,500 graft procedure, a person with 2.4 hairs per follicular unit will have 1,000 more hairs than a person with a density of 2.0. (Figure 7.)
Figure 7. Hair counts in 2,500 graft hair transplants of varying donor densities.
Densitometry, therefore, gives the physician information regarding the number of single hair units that can be anticipated from a given size donor strip (without having to subdivide larger units) and the degree to which the larger follicular units can create central and forward weighting to enhance the aesthetic impact of the procedure.
Donor Miniaturization
Normally, the donor area shows little or no miniaturization and the density counts described above are useful in predicting both the short- and long-term outcome of the procedure. However, if genetic hair loss affects the donor area, the situation changes dramatically. Once full-thickness terminal hair begins to miniaturize, the cosmetic value of the follicular unit begins to decrease and the value of the grafts will be diminished. In other words, just because hair is transplanted, it doesn’t make the hair transplant permanent – the hair in the donor area must be permanent.
Early detection of miniaturization in the donor area is a warning sign that the donor area is not stable and that the person may not be a good candidate for surgical hair restoration. If any miniaturization is detected in a young person, i.e. under the age of 25, red flags should go up that their donor area may not be stable. When miniaturization is noted in a teenager, the risk of developing diffuse unpatterned hair loss (see below) is significant. In an older adult male, some miniaturization, perhaps up to 20%, is consistent with being a good surgical candidate.
Unlike men, adult women often have significant levels of miniaturization in the donor area, so the mere presence of miniaturization is not necessarily a contraindication to surgery. However, miniaturization does indicate an unstable donor supply and one has to make a judgment regarding the risk/reward of the procedure. The physician needs to consider the absolute number of full terminal hairs that are available for the hair transplant, the risk of further miniaturization, the area that needs to be covered, and the risk of the surgery accelerating the hair loss. This is particularly important to consider in women, since hair is often transplanted into an area that has a considerable amount of existing hair – some of which is at risk of being shed from the surgery.
In women, when the risk of continued miniaturization of the donor area is added to the risk of the surgery accelerating hair loss in the area to be transplanted, a far fewer percentage of women are good candidates for surgery compared to men. To think otherwise is disingenuous.
Diffuse Patterned and Un-patterned Alopecia
The importance of donor miniaturization as a factor affecting a person’s candidacy for a hair transplant was emphasized almost a decade ago in the paper “Follicular Transplantation: Patient Evaluation and Surgical Planning.”4 In this writing, we described two conditions; “Diffuse Patterned Alopecia” (DPA) and “Diffuse Unpatterned Alopecia” (DUPA). These were first mentioned by O’tar Norwood when he devised the classification of androgenetic alopecia that bears his name. These two conditions, however, were not detailed in his paper and never received much attention. This was unfortunate because their understanding gives important insights into how to determine who will be a candidate for hair restoration surgery.5
Diffuse Patterned Alopecia (DPA) is characterized by diffuse thinning (miniaturization) in the front, top, and vertex of the scalp in conjunction with a stable permanent zone. DPA is usually associated with the persistence of the frontal hairline and, in the early stages, the thinning is relatively even across the top of the scalp. This contrasts with regular Norwood patients that have early hair loss at the temples and in the crown with balding that spares the top of the scalp. Patients with DPA can be good candidates for hair transplantation due to their stable permanent zone; however, they have an increase risk of shedding after the hair transplant, due to the diffuse miniaturization across the top of the scalp.
In the less common Diffuse Unpatterned Alopecia (DUPA), the miniaturization process occurs over the entire scalp, so that the person lacks a stable permanent zone. People with DUPA tend to lose their hair at an early age, often beginning in their teens. In the early stages, there may be only a slight suggestion of decreased hair volume overall and actual thinning may only be noted through densitometry. Over time, the back and sides of the scalp can take on a transparent appearance, particularly when the hair is cut short. Because the donor area is not permanent, hair transplantation is contraindicated in patients with Diffuse Unpatterned Alopecia.

Figure 8 (left image): DUPA, Age 24, 50% miniaturization Donor Density = 1.2 hairs/mm2
Figure 9 (right image): DUPA, Age 20, 80% miniaturization Donor Density = 1.6 hairs/mm2
Although fully manifest diffuse unpatterned hair loss is relatively uncommon in men, there are many younger patients who have slightly increased degrees of miniaturization in the back and sides of the scalp, making the long-term stability of the donor area questionable. In these patients, the decision to recommend hair restoration surgery is particularly difficult. As a general rule, if the decision is difficult, it is best postponed, since, over time, the stability of the donor area will become more obvious. A mistake can leave the patient with transplanted hair that will thin over time and a donor scar(s) that may become visible.
Both Diffuse Patterned and Unpatterned alopecia also occur in women. However, in contrast to men, the DUPA pattern in women is much more common, possibly occurring 10 times as frequently as DPA. As in men, female patients with DUPA are not good candidates for a transplant, except in the instance where the goal is solely to soften the frontal edge of a hairpiece. The high incidence of Diffuse Unpatterned Alopecia in women partly explains why many fewer women are good candidates for hair transplantation as compared to men.
It is important to emphasize that other, non-genetic, causes of hair loss must be considered in cases where the balding pattern is diffuse. These include anemia, thyroid disease, connective tissue disease, gynecological conditions, severe emotional events, and medications. Although the presence of miniaturization likely points toward a hereditary cause of the hair loss, with diffuse hair loss other etiologies must always be entertained.
Conclusion
Densitometry is an important tool for the evaluation of hair loss and for assessing candidacy for hair transplantation. Measuring donor density and assessing the degree of miniaturization in the donor area should be an integral part of the evaluation of every patient in which surgical hair restoration is considered. This will enable physicians to better select those who are good candidates for a hair transplant and help identify those patients in whom the procedure is contraindicated. For patients having a hair transplant, these measurements will enable the physician to better estimate the size of the donor strip and be better able to anticipate the aesthetic outcome of the hair restoration procedure.



