
Robert M. Bernstein, M.D., Michael B. Wolfeld, Gabe Zingaretti, PhD
Hair Transplant Forum Intl. 2014; 24(3): 95-97.
The initial application of the ARTAS® robotic system (robot), released in the fall of 2011, was the separation of follicular units from the surrounding scalp tissue, the first step in a follicular unit extraction procedure. ((Canales MG, Berman DA. The age of surgical robots. Hair Transplant Forum Intl. 2008; 18(3): 95-96.)), ((Bernstein RM. Integrating Robotic FUE into a hair transplant practice. Hair Transplant Forum Intl. 2012; 22(6): 228-229.)) Subsequent steps in FUE include removal of the follicular unit grafts from the donor scalp, site creation, and graft placement. With its new hardware and software capabilities, the robot can now perform one more step in this process, making recipient sites. Preliminary observations suggest that it can accomplish this function with greater precision and consistency than when performed manually.
For robotic recipient site creation, the doctor first draws a hairline and other markings directly onto the patient’s scalp to delineate the recipient area. Next, multiple photographs are taken of the patient and, using new software called the ARTAS Hair Studio™, the images and markings are converted into a 3-D model of the patient. The robot uses the inter-pupillary distance (IPD) to match dimensions of the model with the actual dimensions of the patient.
To determine how the hair will ultimately grow, the physician uses the software to specify the angle of the recipient site incisions (relative to the plane of the scalp), incision direction, site depth, average density, and total number of incisions. The site spacing can then be easily modified to create variations in density in different parts of the scalp while the computer keeps the total number of sites constant.
An important feature of the ARTAS® system is that the robot uses image-guided technology to avoid hairs of a specific diameter when making recipient sites. In this way, the distribution of sites that are created in the procedure can be made to complement the distribution of existing terminal hairs (or the hair from prior hair transplant procedures), while ignoring hair that is miniaturized or vellus. The physician can specify the cut-off diameter based upon the diameter of the patient’s full terminal hairs. Partially miniaturized hair may also be included in the group of hairs to be avoided. Once this parameter is set, the robot will proceed to create sites at a minimum distance from the selected existing hair and do so randomly throughout the areas where the hair is finer or the scalp is bald.
The imaging software is currently used to translate the design the physician makes directly on the patient scalp into a computerized algorithm that directs the creation of recipient sites in the operating room. In the future, the system will also have the capability of simulating, in advance of the surgery, what the actual hair transplant will look like so that it can be used as tool to aid the physician during the consultation.
Case Study
Patient YM is a 44 y/o, white male, with straight, fine, brown hair with a Norwood Class 6/7 pattern of hair loss. His donor density is 70 FU/mm2 and he has 20% donor miniaturization. After discussing the various surgical modalities for hair restoration, the patient chose FUE in order to wear his hair relatively short. He understood that due to his extensive hair loss and limited donor supply, the goal was to restore light coverage to the front and top of his scalp. The ARTAS™ system would be used for both follicular unit dissection and recipient site creation. To minimize the time the grafts were outside the body, recipient site creation would be performed before graft harvesting. ((Bernstein RM, Rassman WR. Pre-making recipient sites to increase graft survival in manual and robotic FUE procedures. Hair Transplant Forum Intl. 2012; 22(4): 128-130.))
The morning of surgery the procedure was reviewed, consent was obtained, and five photos were taken; full-face front, top of scalp, back of scalp, and left and right sides. The photos were then loaded into the ARTAS Hair Studio™ software. Using facial landmarks – eyes, nose, mouth, forehead, and chin – as a guide, a 3D model was built around the images and was displayed on a touch-screen monitor. The IPD measured 63.4mm. The recipient site parameters were then specified. The recipient site depth was programmed at 5.5-mm with an angle of elevation from the scalp of 45 degrees. All of the sites were programmed to 0 degrees, meaning that they would point in a forward direction and be parallel to each other. The robot was programmed to avoid hairs with a diameter of 80u or greater. (Figure 1)
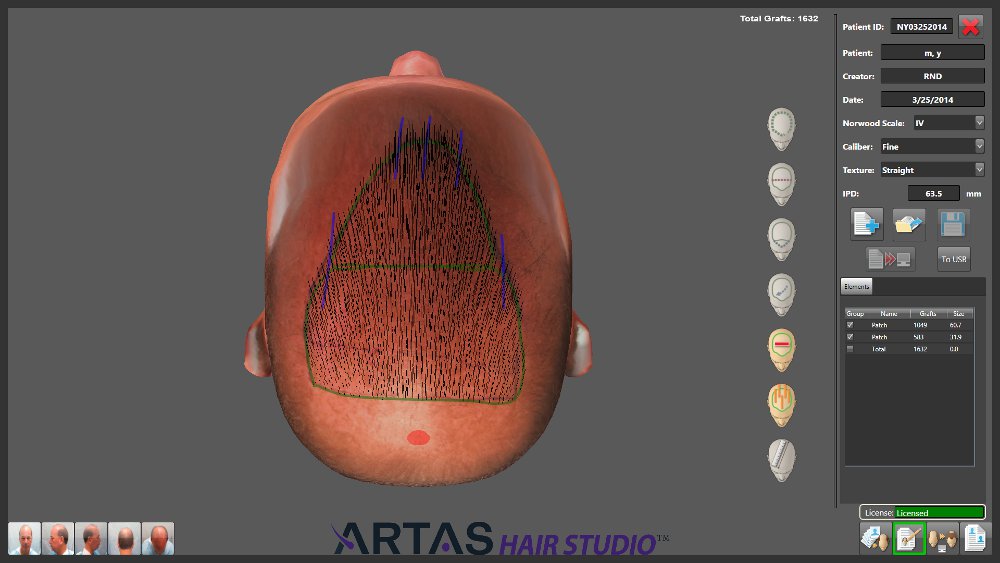
Figure 1. ARTAS Hair Studio™ software showing the hair transplant design
Vital signs were taken and a pulse oximeter was attached to the patient’s left middle finger. The patient was sedated with oral valium and IM versed. Local anesthesia was administered using a ring-block consisting of xylocaine 0.5%, bupivicane 0.25% and epinephrine 1:200,000.
The robotic harvest and subsequent dissection yielded 2,256 grafts consisting of 228 1s, 1144 2s and 884 3s. All forty 4-hair grafts were dissected under a stereo-microscope into smaller grafts (3s and 1s) to generate enough 1s for the frontal hairline and to ensure a natural appearance in a patient with low overall density.
Using a 19-gauge hypodermic needle to make the incision, the robot created 1,632 recipient sites. In Area 1, the frontal region of the scalp measuring 32 cm2, 583 sites were created at a density of 18.2 grafts/cm2. In Area 2, the mid-scalp measuring 61 cm2, 1,049 sites were created at a density of 17.2 grafts/cm2. The remaining 624 recipient sites were made by hand; 220 for the frontal hairline and the remaining 404 for the transition zone in the posterior aspect of the mid-scalp and to fill in gaps.
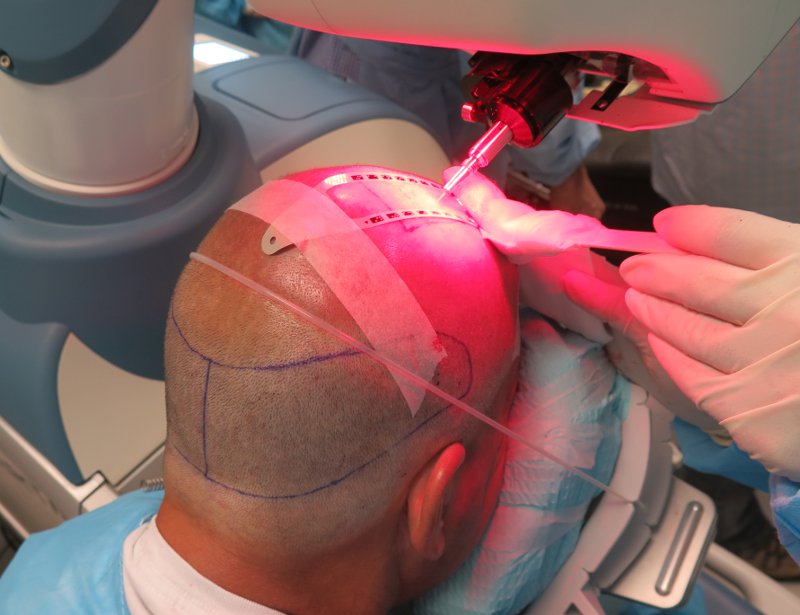
Figure 2. Creating recipient sites with the ARTAS® robot
The current system uses a grid, measuring 2.5cm x 13cm, that is placed vertically on the patient’s scalp. This serves to orient the robotic optical system. (Figure 2) After the grid is filled with recipient sites, it is moved to a new position adjacent to the first. In the current procedure, the robot created sites at 1,500/hr. With time for set-up and moving grids and creating the manual sites, the total time for site creation was 1.5 hours. (Figures 3, 4)

Figure 3. Before with marking for the procedure

Figure 4. Two days post-op
Discussion
As with the extraction process, the robot eliminates the inconsistencies inherent in creating large numbers of recipient sites by hand. The robot can create sites at a rate of up to 2,000 per hour, although there is more set-up time compared to sites made manually. The physician can specify punch depth (3.5 mm to 7mm), punch angle to the scalp (35 to 60 degrees), and site direction (forward, parallel, lateral, etc.). Once these parameters are set, site creation is precise and rapid.
The case described above was the first time we used the robot to create recipient sites on the front and mid-scalp. Cases subsequent to this have shown that there is a rather quick learning curve that results in a reduction in the time needed for data input, set-up, and grid placement; and a shorter overall duration for this step of the hair transplant procedure.
One of the benefits of robotic site creation is that the distribution of grafts over a fixed area of the scalp can be exact. For example, if one wants to transplant 1,000 grafts evenly over 50cm2 of area, this can be done with great precision and with uniform site spacing. In addition, the physician can vary the densities in select regions of the scalp and the robot will adjust the densities in other areas (in real time) so that the total number of sites remains the same. For example, if one has 2,500 follicular units to cover 120cm2 of scalp and wants to create a density of 25 sites/cm2 in a 40cm2 frontal forelock and use the remaining grafts to cover the other 80cm2 of bald scalp, the robot will automatically calculate a second density of 18.75 sites/cm2 for the remaining area.
Another benefit is that the robot can be programmed to avoid existing hair and select which specific hair diameters to avoid. The robot is programmed to keep a minimum distance from the existing hair of at least 250 microns (or greater with lower target densities) to ensure that the resident follicles will not be damaged and that the distribution of new hair is even and natural. This computerized mechanism appears to be more accurate than what can be done by hand and does not sacrifice speed in the process. This is an important benefit of the new technology.
Compared to manual FUE, the disadvantage of making sites with a robot is the additional set-up time and small additional cost (if one is already is using the robot for extraction). The disadvantages of robotic site creation when performing FUT procedures include cost, the need for a dedicated room, additional staff training, and set-up time. Another issue involves the preparation for site creation. When creating recipient sites, the recipient area must be clipped to 1-mm in length. In FUE, the patient often prefers this length to match the donor area which has already been clipped. Since the donor clipping is not necessary in FUT, these patients generally prefer to keep any hair they have in the recipient area uncut. Therefore, only FUT patients who are already bald in the recipient area would choose to have their sites made by the robot. Because of these constraints, robotic site creation lends itself more to robotic FUE procedures and will probably be used less often in FUT procedures, even if there is a robot on the premises. A final issue is that using a robot for site creation may be impractical for very small sessions that can easily be accomplished by hand.
At this time, the robot is not capable of making the necessary directional changes needed to reproduce the natural swirl that occurs in the crown. In addition, although the robot can be programmed to create a hairline, the nuanced irregularity of the hairline lends itself to being done by hand. If the robot is used for this part of the procedure, a change to a smaller needle is required to accommodate the single-hair grafts.
For the physician who is skilled at follicular unit hair transplantation (either by FUE or FUT), robotic site creation adds modest value to the procedure, as recipient site creation is perhaps the easiest step to perform. A more significant benefit of the new technology is in the imaging tool that can assist the physician in showing the patient the outcome of the procedure in advance of the actual surgery. Of course, its greatest value is that automated site creation is a necessary precursor to the final step of a completely robotic hair transplant, automated graft insertion – a technology is at least several years away.
Summary
In performing recipient site creation, the robot automates another part of the hair transplant process that can be prone to human error and variability. In addition, the new technology will soon give the physician a consultation tool to show what the hair restoration procedure can do and to help align the patient’s expectations with anticipated results.
Probably the greatest significance of this new method of site creation is that it brings the technology one step closer to the goal of a totally automated hair transplant that that can be performed with robotic precision, speed, and reproducibility. The physician can then focus on the critical, but more subjective, elements of the hair restoration process; namely patient selection, patient education, and hair transplant design.
Dr. Bernstein is a medical consultant to Restoration Robotics, Inc. Dr. Zingaretti is head of research and development at Restoration Robotics, Inc. Drs. Bernstein, Wolfeld, and Zingaretti have financial interests in the company.



