
A New Surgical Instrument For the Automation of Hair Transplantation
WILLIAM R. RASSMAN, MD, Los Angeles, CA
ROBERT M. BERNSTEIN, MD, New York, NY
Dermatologic Surgery 1998; 24: 623-627.
Hair transplantation in the 1990’s has rapidly evolved from a simple 1 to 2 hour procedure, easily accomplished by a physician and one or two assistants, into a labor intensive, 3 to 10 hour “megasession” procedure, involving the movement of hundreds to thousands of grafts in a single sitting, requiring a large coordinated team of highly trained staff. ((Bernstein RM, Rassman WR, Szaniawski W, Halperin AJ. Follicular transplantation. Int J Aesthet Rest Surg 1995; 3:119-132.)) These techniques have produced extremely natural looking hair transplants that can be achieved in just a few treatment sessions. However, the technical difficulties and issues of quality control have proved to be a significant problem, even for the most experienced transplant teams.
As the number of technicians and medical assistants involved with the procedure increases, so do the problems of organization, management, and quality control. With a large staff, insuring that the technical aspects of the procedure are carried out with uniformity and precision becomes a major concern of the physician. As the number of implants moved per session increases, so do the problems associated with graft desiccation, warming, and survival, since the implants must now be kept outside the body for longer periods of time. Also increased are the problems associated with the tedium of filling hundreds to thousands of recipient sites. Staff fatigue and decreased attention spans can result in missed sites, piggybacking, and trauma to the grafts.
Large sessions of closely spaced sites also pose additional problems of hemostasis and graft popping, all of which contribute to an increased risk of mechanical injury. A well-trained technician will carefully grasp the graft by the fat below the bulb, or the connective tissue beside the follicular structure. However, once a second pass is needed to reinsert or re-position a partially placed graft, especially with decreased visibility from even minor amounts of bleeding, problems arise. The grafts are no longer held carefully by the edge, but often hastily grabbed across their surface, traumatizing the growth elements and possibly causing permanent injury to the implants. ((Greco J. Is it X-factor or H-factor? Hair Transplant Forum Int 1994; Vol. 4, No. 3:10-11.)), ((Greco J. The H-factor in micrografting procedures. Hair Transplant Forum Int 1996; Vol. 6, No. 4:8-9.)), ((Cooley, MD, Jerry: Loss of the dermal papilla during graft dissection and placement: Another cause of X-factor? Hair Transplant Forum International 1997; Vol. 7, No. 1:20-21.))
A new disposable instrument, the Rapid Fire Hair Implanter Carousel (Carousel), has been developed which automates two of the most difficult and labor intensive components of the hair transplant process; the creation of the recipient sites and the insertion of the implants. These two steps can now be performed in rapid sequence and in one simple motion. The implants are stored in a cartridge while they await placement. Large numbers of implants can then be placed in a relatively short time span, decreasing both the length of the surgery and the requirement for a large staff. The instrument reduces the risk of damage to the implants from desiccation and manual manipulation. The instrument can be used equally well for micrografting ((Rassman, WR, Carson S. Micrografting in extensive quantities. The ideal hair restoration procedure. Derm Surg 1995; 21:306-311.)) or for Follicular Transplantation,1, ((Bernstein RM, Rassman WR. Follicular transplantation: patient evaluation and surgical planning. Derm Surg 1997)), ((Bernstein RM, Rassman WR. The Aesthetics of follicular transplantation. Derm Surg 1997)) although these authors feel that a superior cosmetic results will be obtained if the Carousel is loaded exclusively with follicular units, rather than with micrografts cut to size.
This paper describes the new instrumentation and examines its use in a single case study.
Materials and Methods
A 34 y/o Caucasian male with a Norwood Class IIIa, male pattern alopecia volunteered for this study. The patient had dark brown hair of average diameter, medium colored skin, and had a donor density measuring 2.8-3.0 hairs/mm2. He showed normal levels of donor site miniaturization and his scalp laxity was average. The surgical plan was to restore his frontal hairline and to add coverage to the front part of his scalp.
After consent forms were signed and pre-operative photographs taken, the patient was pre-medicated with Celestone IM, dicloxacillin 500mg PO, and diazepam 10mg PO. The hair in the mid-portion of the permanent zone was clipped to a length of 1.5 mm. Local anesthesia, containing a mixture of 40% bupivicane, 60% lidocaine, and 1/200,000 epinephrine was administered in a ring block fashion to the donor area. A single donor strip was harvested with two parallel blades set 1.5 cm apart on a Rassman Handle. The donor area was closed with a single running 2-0 chromic suture. The donor strip was dissected into 1,200 implants consisting one-, two-, and three-hair follicular units. Four hundred units were temporarily placed in chilled saline and then loaded into the Carousel cartridges (see below) which was then sealed awaiting use. Eight hundred implants were stored in chilled saline to be used with the manual placing technique. The dissection was carried out using 2-4x magnification with the aid of transillumination. ((Rose, P: Presentation, American Hair Restoration Society Meeting, AACS, Orlando, Florida, Jan 1996.)) Both groups were prepared in an identical manner except that during dissection the superficial portion of the epidermis was removed from the implants that were to be used in the Carousel.
Four hundred follicular units were transplanted with the Carousel into the test site, which consisted of an area on the right side of the patient’s scalp approximately 1cm behind the right frontal hairline. The remainder of the frontal area on the right side and the entire contralateral side, serving as a control, was transplanted with 800 follicular units using manual techniques. This consisted of using an 18g NoKor needle to create the recipient sites and jeweler’s forceps to manually insert the implants.1,7
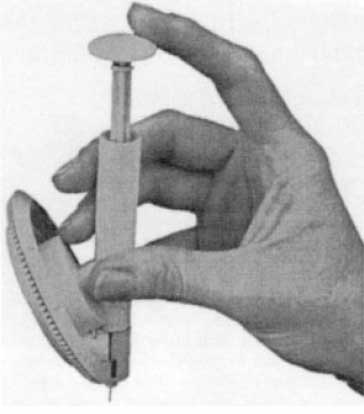 Figure 1. The Rapid Fire Hair Implanter Carousel
Figure 1. The Rapid Fire Hair Implanter CarouselThe Rapid Fire Hair Implanter Carousel was used for the test area. This instrument is a disposable, hand held mechanical device (see figures 1 and 2). The Carousel has a sharp end designed to pierce the scalp, an insertion element to move the implants into the recipient site, and a button end that is the activator of the mechanical components. The button end is similar to the activation button of a ball point pen. A circular cartridge is located in the central portion of the Carousel which houses the individual follicular grafts. When placed in the cartridge, the grafts are oriented with the skin surface facing toward the center of the cylinder, and the hair bulb facing outward. Each cartridge is designed with 100 cylindrical slots to house 100 micrografts or follicular implants. The cartridge is secured onto the Carousel with a locking ring.
 Figure 2. The Carousel in Position
Figure 2. The Carousel in PositionThe loaded instrument is held between the thumb and the middle and ring fingers. In a short, quick downward motion, the cutting edge at the tip of the Carousel is made to penetrate the patient’s scalp creating a tiny slit for the implant. The angle of penetration is at the discretion of the surgeon. The index finger activates the instrument by placing pressure on the button on top of the Carousel. This allows the mechanical components of the instrument to pick up a graft from the chamber. As the graft continues down its path, it is carried through a needle bore into proper position in the patient’s scalp. The instrument is withdrawn, leaving the graft in place. It is then moved to a new position on the scalp. The Carousel functions so that the placing of one implant automatically advances the next implant into position. Four Carousels, loaded with 100 implants each, were used for the test area.
 Figure 3. (A) Once the grafts are harvested, they are placed into slots of a cartridge. Small droplets of saline are placed with the grafts. (B) Once the slots are filled, a cover is placed over the cartridge and the entire apparatus is refrigerated until the grafts are implanted.
Figure 3. (A) Once the grafts are harvested, they are placed into slots of a cartridge. Small droplets of saline are placed with the grafts. (B) Once the slots are filled, a cover is placed over the cartridge and the entire apparatus is refrigerated until the grafts are implanted.NOTE: The Carousel functions in a manner similar to other tools used in the hair transplant process such as trochars, punches, and knives, which create openings in the scalp. Any instrument used to penetrate the scalp can also penetrate the skull if significant forces are applied. A skilled hair transplant surgeon must determine the amount of force that is applied, so that the skull is not penetrated. The depth of penetration can be determined by observation and by contact with the bony skull. The physician must use his judgment in determining both the depth and the force that must be applied to make the opening in the recipient area of the scalp. Prior to use on the scalp, the physician must assess the integrity of the bony skull. If any defects in the bony skull are present, or suspected, the physician must not proceed without further evaluation.
Results
The Carousel incorporates a one-step approach that was used for the site creation and placement of the 400 grafts transplanted to the right side of the study patient’s scalp. It produced visibly less bleeding overall when compared to the manual two-step approach (using a Nokor needle and forceps). Since the Carousel inserted the grafts as the sites were made, the implants appeared to tamponade the bleeding from those recipient sites. In contrast, with the conventional Nokor needle that was used for the remaining 800 grafts, the sites were made and left open until hemostasis was complete and all of the sites were created.
In the manual technique, many of the implants were manipulated several times as they were re-grasped. This was especially evident if bleeding caused poor visibility. In addition, implants that were elevated from bleeding (or popping) had to be re-inserted or adjusted.
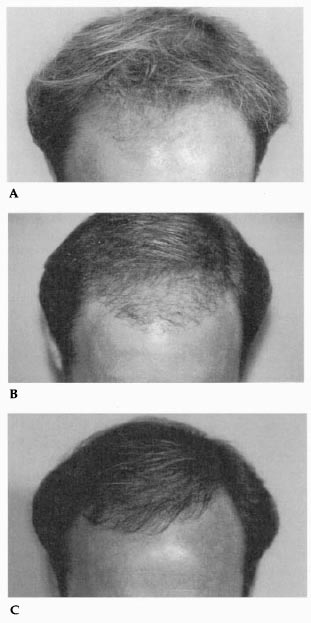 Figure 4. (A) Before and (B) 4 months post-op; (C) 8 months post-op.
Figure 4. (A) Before and (B) 4 months post-op; (C) 8 months post-op.The Rapid Fire Hair Implanter Carousel, which created the recipient sites and implanted the grafts in one step, took approximately 10 minutes (40 grafts/minute). With the manual technique, placement of the equivalent 400 implants took 1 hour (6.6 grafts/minute). The remaining 400 grafts took an additional hour. We used our most experienced technician to place all of the manual grafts, in order to minimize the human variables in the control group.
Post-operative wound examination showed no difference between those sites made with the Carousel and those made with the conventional trochar. An independent observer felt that they were similar with respect to the rate of healing as indicated by the time it took for the crusting to disappear (approximately 6 days), and the time for the erythema to fade (approximately 3 days).
Healing and hair growth were followed by serial photography. Photographs were taken before surgery (see figure 3), and then at the following intervals: 1 day post-op, 2 days post-op, 3 days post-op, 9 days post-op, 1 month post-op, 2 months post-op, 3 months post-op, and 4 months post-op (see figure 4).
In viewing the photographs, or directly viewing the patients, there was no difference observed between the site healing or graft growth when the Carousel and manual techniques with compared. The first significant growth wave commenced at about 90 days following surgery in both sides. When identical size areas in the test and control sides were compared, there was no difference noted in the total amount of hair observed at 4 months.
Discussion
The purpose of this paper is to introduce the Rapid Fire Hair Implanter Carousel. The major advantages of the Carousel are:
- The Carousel is able to simultaneously create sites and insert the implants in approximately the same time it takes the surgeon using the manual method to make the sites alone. Since the placing of implants into pre-made sites has been the most time consuming part of the manual transplant procedure, the elimination of this step greatly reduces the total operative time.
- The skilled staff needed to insert the implants (the most labor intensive and difficult part of the transplant procedure) can be reduced significantly.
- In performing larger transplant procedures with the manual process, grafts must often remain outside the body for hours awaiting placement. With the Carousel, this time is reduced significantly, since the grafts are implanted at the same time the sites are made. This reduces the risk of damage from desiccation and warming. It also theoretically minimizes the chance of poor graft growth, by decreasing the time the grafts are separated from their blood supply.
- Human manipulation of the grafts during the insertion process in the manual technique has been a significant source of injury to the implants, since the grafts are often inadvertently squeezed and/or crushed by the placer’s forceps. This is often compounded by the decreased visibility caused by bleeding from the sites prior to and during graft insertion. Since the Carousel completely bypasses this step in the procedure, this potential source of graft injury can be greatly reduced or eliminated.
The conclusions that can be drawn from a single case study that lack true bilateral controls are obviously limited. Ongoing clinical trials will be conducted by these authors on additional patients and under a more formal protocol as more instruments become available. Although this pilot study involved the placement of only 400 test implants, it seems clear that the instrument significantly simplifies the hair transplantation procedure and will be equally versatile when several thousand implants are used in a single session since several individuals can use different Carousels simultaneously.
The actual quantitative advantage that automation holds in the implantation process by bypassing the need for “human placers” is still speculative. What this case study shows is that in one patient, under ideal conditions, the instrument compares favorably to the manual technique. Besides speeding up operative time and reducing staffing requirements, the elimination of some of the human factors contributing to graft injury certainly presents a compelling argument to use this new instrument. Studies comparing the Carousel to that of the manual technique using objective measurements of hair growth, under strict bilateral controls and in multiple patients, must still be performed. These studies would, of course, be best performed by researchers not involved in the development of the instrument.
Conclusion
Preliminary results from a single pilot study proved that the partial automation of the hair transplant process is technical feasible. It showed that the Rapid Fire Hair Implanter Carousel has the potential to significantly reduce the operative time of a hair transplant, decrease staffing requirements, and minimize the risk of iatrogenic trauma to grafts during the implantation part of the procedure. The benefits that this new technology may offer in surgical hair restoration still need to be explored in well-controlled studies.



