
Robert M. Bernstein, M.D., William R. Rassman, M.D., and Nazia Rashid
Dermatologic Surgery 2001; 27(1): 5-11.
College of Physicians and Surgeons, Columbia University, New York, New York
THE IDEAL SUTURE should be strong, handle easily and form secure knots. The ideal wound closure should ensure hemostasis, have a low risk of infection, be comfortable for the patient, and result in a fine surgical scar. ((Bennett RG: Selection of wound closure materials. J Am Acad Dermatol 1988; 18: 619-37.)), ((Moy RL, Waldman B, Hein DW: A Review of Sutures and Suturing Techniques. J Dermatol Surg Oncol 1992; 18: 785-95.)) A fine scar in the donor region following a hair transplant is especially important since it gives patients flexibility in styling and the option to wear their hair relatively short. It also allows for efficient harvesting of hair in subsequent procedures, thus maximizing the total donor supply.
The most common type of donor closure in hair transplantation is with non-absorbable, running sutures, usually of nylon or polypropylene (Prolene, Surgilene). This is accomplished with, or without, buried absorbable sutures, usually of polyglactin 910 (Vicryl) or Polyglycolic acid (Dexon). This method of closure provides good control of wound edges and is relatively fast, especially when moderate to large bites are used. Larger bites keep the sutures from becoming buried during the healing phase and make their removal easier.
In spite of their popularity, there are several problems associated with this type of closure. The running suture has the tendency to strangulate tissue and compromise the blood supply to the wound edges. This can be problematic when the closure is under tension or when there is a significant amount of edema. The involved tissue will heal more slowly and may be more subject to infection. In addition, the hair follicles incorporated within the sutures may be shed and this hair loss may be permanent. Finally, although synthetic non-absorbable sutures have low tissue reactivity, they can cause mechanical inflammation if there is any tension on the wound.
To minimize tissue strangulation, a running suture may be used with the bites placed very close to the wound edges. However, the problem with this technique is that, as healing progresses, the sutures quickly become buried and difficult and traumatic to remove. To circumvent the removal issue, absorbable sutures have been used in the cutaneous running stitch. Unfortunately, the commonly used absorbable sutures (gut, chromic, Vicryl and Dexon) all incite a considerable inflammatory reaction in the skin and this inflammation can be associated with permanent alopecia along the suture line.
The purpose of this study is three-fold. First, to describe the use of Poliglecaprone 25 (Monocryl), a synthetic, absorbable, monofilament suture ((Bezwada RS, Jamiolkowski DD, Lee I-Y, et al: Monocryl suture, a new ultra-pliable absorbable monofilament suture. Biomaterials 1995; 16: 1141-48.)), ((LaBagnara Jr. J: A review of absorbable suture materials in head and neck surgery and introduction of Monocryl: a new absorbable suture. ENT J 1995; 74(6): 409-15.)) in hair transplantation surgery. Second, to detail the suturing techniques needed to maximize the benefit of this suture. Third, to compare this material and suturing technique to another type of closure, that of metal staples.
Poliglecaprone 25 has the chemical structure (C2H2O2)m(C6H10O2)n, which forms a complex polymeric chain giving Monocryl its special properties. The monofilament is comprised of a soft segment that consists of a random co-polymer of -caprolactone and glycolide that provides good handling characteristics. A hard segment, composed of polyglycolide, gives the suture its strength.3 As a result; the suture possesses excellent handling and knot security, minimal resistance as it passes through tissue, and the highest tensile strength as compared to other absorbable monofilament sutures.3,4, ((Nahai F, Bried JT: Evaluation of the Monocryl suture for skin closure in 100 plastic surgery patients. Perspectives in Plast Surg 1995; 9(1): 1-4.))
Poliglecaprone 25 has been shown to be non-toxic and non-allergenic and without pyrogenic or hemolytic potential.3 The synthetic material is slowly broken down by the body via hydrolysis and therefore incites little inflammatory reaction in the skin. The reduction in the tensile strength of Monocryl, as it is absorbed over time, is consistent with the requirements of most hair transplant surgery procedures3,4 (Table 1).
Stainless steel staples were chosen for the comparison since they have the advantage of being totally inert, not causing tissue strangulation, being fast to apply, and having been reported to result in excellent healing. ((Stegmaier, OC: Use of skin stapler in dermatologic surgery. J Am Acad Dermatol 1982; 6: 305-9.)), ((Stough DB, Haber RS. Hair Replacement: Surgical and Medical. St. Louis: Mosby-Year Book, Inc., 1996: 136-7.))
We performed a bilateral controlled study designed to compare donor wound closure using Poliglecaprone 25 sutures (Monocryl) with a closure using stainless steel staples. Patients were evaluated with regard to post-operative course, resultant surgical scar and suture preference. We will also discuss some of our clinical experience in using this new suture material.
Methods and Materials
Follicular Unit Transplantation was performed on 22 adult male volunteers; in sessions ranging from 600 to 2500 grafts using previously published methodology. ((Limmer BL. Elliptical donor stereoscopically assisted micrografting as an approach to further refinement in hair transplantation. Dermatol Surg 1994; 20: 789-93.)), ((Bernstein RM, Rassman WR: Follicular Transplantation: Patient Evaluation and Surgical Planning. Dermatol Surg 1997; 23: 771-84.)), ((Bernstein RM, Rassman WR: The Aesthetics of Follicular Transplantation. Dermatol Surg 1997; 23: 785-99.)) All patients were undergoing their first hair transplant procedure. Donor anesthesia was established with a ring block of 10-15cc of a solution containing 60% Lidocaine 0.5%, 40% Bupivicaine 0.25%, and 1:200,000 epinephrine. Donor tumescence was achieved by infiltrating 20-30cc of Lidocaine 0.17% with 1:600,000 epinephrine into the subcutaneous space using 10cc syringes and 25g needles.
Approximately 2-3 minutes after the tumescent mixture was administered, a donor strip was harvested using two parallel blades set on a Rassman handle 1.2cm – 1.5cm apart. (The handle pre-angles the blades at 30o to follow the direction of the emerging hair). In the protocol procedures, the strip widths ranged from 0.9 to 1.3cm and the lengths from 6 to 25cm (measurements taken after the strips were harvested). The ends of the donor strip were equidistant from the midline.
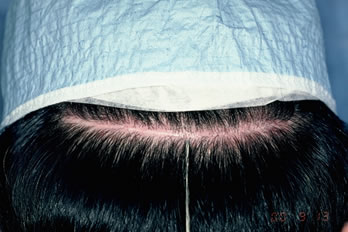
One side of each donor area was closed with Poliglecaprone 25 suture (Monocryl 4-0, PS-1 cutting needle, 70cm length, Undyed) (Figure 1.). The contra-lateral side was closed with stainless steel staples (3M-Precise DS-25) (Figure 2.).
 Figure 1. 4-0 Monocryl Suture.
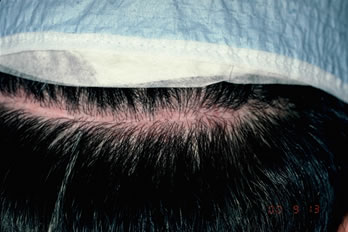
Figure 1. 4-0 Monocryl Suture. Figure 2. Precise DS-25 Stapler.
Figure 2. Precise DS-25 Stapler.On the sutured side, a single running 4-0 Monocryl suture was used. The bites were spaced approximately 0.5cm apart and the suture was advanced on the surface, rather than under the skin (as in traditional surgery), in order to minimize the amount of suture in contact with the follicles (see discussion section). The needle was passed through the full thickness of the dermis and exited the wound edge just below it (at the level of the bulbs) without incorporating any significant amount of subcutaneous tissue. The needle track was kept parallel to, and within 1.5mm of the wound edge (Figures 3A, B).
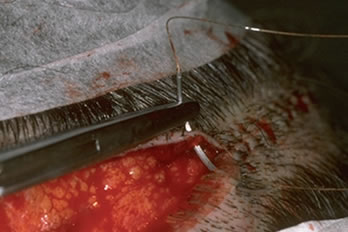
Since the upper wound edge is cut at a 30o angle, the needle must penetrate the skin with an “upward” motion (with the patient in a sitting position) so that the needle remains parallel to the wound edge though its entire course through the tissue. Occasionally, the upper wound edge will be distorted by the elastic retraction of the dermis so that the upper wound edge may require slight eversion with rat-tooth forceps for proper suture placement. This is usually not required for the lower edge where needle placement is easier.
The wound edges on the stapled side were approximated with a skin hook grasping the lower edge and rat toothed forceps grasping, and slightly everting, the upper edge (This required the help of an assistant). Once the wound edges were flush, the staples were applied in such a fashion that the middle of the staples rested slightly above the incision line. This permits a better grasp of the upper wound edge whose edge is thinner due to the acute angle of the blades. The staples were placed approximately 0.6cm apart. (Figure 4.)

Patients were evaluated for post-op complications, discomfort, and resultant surgical scar. Recorded observations were made on follow-up visits 10-14 days (Figure 5.) and 6-8 months post-op. Staples were removed at the 10-14 day post-op visits. The sutures were left in place. Post-op complications and post-op discomfort were assessed via questionnaires filled-out by the patients at the time of their follow-up visits. The surgical scar was evaluated subjectively with questions on donor area cosmesis and objectively by measuring the width of the donor scar at multiple points along the suture-line. Finally, all patients were asked the question, “Which suture would you prefer to be used in future procedures?”
 Figure 5. Appearance of a typical closure at 12-days post-op.
Figure 5. Appearance of a typical closure at 12-days post-op.Results
The results of the 22 patients in our study are summarized in Table 2. The following post-operative complaints were reported on the staples side; tenderness (12 patients), itching (4 patients), swelling at the suture line (2 patients) and scabbing (1 patient). This compared to two post-op complaints from the Monocryl side; itching (1 patient) and swelling (1 patient).
Of the 22 patients studied, one patient reported post-op bleeding on the staples side and one noted it on the sutures side. Further questioning, however, revealed that these patients had only experienced some blood on the post-op dressing. There was never any active bleeding noted by any patient in the study, any that required intervention on the part of the patient, nor any that prompted a call to the physician. There was no infection or wound dehiscence on either side.
Since it was difficult for patients to directly assess their donor scar, we used an indirect method that we labeled “donor area cosmesis.” This had three components; visibility of the suture material in the immediate post-op period (0-2 weeks), the inability of the patient to wear his hair as short as he had been accustomed to in the more extended post-op period (4-8 months) and, finally, any perceived hair loss along the suture line. Only two patients had post-operative complaints regarding cosmesis, both related to visibility of the actual staples through the hair. No patients had any problems with wearing their hair short in the more extended post-operative period and none had any perceived hair loss from either type of closure.
Donor scars were measured in multiple points to assess the widest, narrowest and average widths. Measurements revealed a wider scar overall on the staples side in six patients and wider scar on the suture side in 2 patients (Figures 6A, B, C). The average scar width on the staples side measured 1.78mm compared to a 1.42mm on the sutures side. (Refer to Table 2 for the average minimum and maximum scar widths from each type of closure.)

The final parameter was a subjective global assessment by the patient regarding suture preference. In response to the question “Which suture would you prefer to be used in future procedures?” 14 of the 22 patients preferred Monocryl, one preferred metal staples and 7 had no preference. The reason behind their choice was explored in more detail in the “comments” section of the questionnaire. Most patients stated that post-operative discomfort from the staples and the inconvenience and occasional pain associated with their removal was responsible for their decision. It is important to note that in the comments section, five patients qualified their answer by stating that, in spite of their preference, they would choose the side that gave the best results when undergoing future procedures.
Discussion
The ideal wound closure should ensure hemostasis, have a low risk of infection, be comfortable for the patient post-op, and result in a fine surgical scar. A fine scar in the donor region following a hair transplant is especially important since it gives the patient flexibility in styling and the option to wear the hair relatively short. It also allows for efficient harvesting of hair in subsequent procedures, thus maximizing the total donor supply.
Since March 1998, we have been closing the donor site of the majority of our hair transplant patients with a single, running cutaneous suture using poliglecaprone 25 (Monocryl). The suture, a synthetic, absorbable, monofilament with low tissue reactivity, appears to have some distinct advantages over other types of materials. We reported our preliminary results with this suture at the International Society of Hair Restoration Surgery, 7th Annual Meeting, San Francisco, CA in October 1999.
Poliglecaprone sutures are made from a co-polymer of glycolide and caprolactone. This synthetic material is broken down by the body via hydrolysis and therefore doesn’t incite the typical inflammatory reaction characteristic of other absorbable sutures. Because of this, the suture can be used to oppose tissue at the level of the hair follicles, without the risk of significant damage to these structures. In addition, the translucent sutures are skin colored and are barely visible once the donor area is sutured closed.
In our experience, carefully harvesting the donor strip by superficial dissection in the mid-fat layer, followed by meticulous approximation of wound edges under little tension, and placing sutures very close to the wound edges, will maximize the chance of a fine scar. A superficial incision that spares fascia will allow for a superficial closure and allow healing without the dermis being bound to the deeper tissues. This will help preserve scalp laxity for subsequent procedures and possibly minimize post-op edema by causing less interference with lymphatic drainage.
Placement of sutures within 1.5 mm of the free edge will provide for excellent dermal to dermal contact and perfect wound edge apposition, without the incorporation of unnecessary tissue and associated hair follicles. This allows the blood supply to reach the edges of the wounds unimpeded and also prevents any post-op edema that might place tension on the sutures and strangulate the tissue. This is especially important in large hair transplant sessions that can be associated with significant amounts of post-operative edema that can compress hair follicles entrapped in the running sutures and cause permanent alopecia (Table 3).
When a running stitch is used in traditional skin surgery, the surgeon advances the suture as it travels through the subcutaneous tissue so that, on the surface of the skin, the visible parts of each loop appear perfectly parallel. Under the skin, however, each suture takes a diagonal course. The reason for this is twofold. The first is to have a more organized “neater” appearance and the second is to minimize any suture marks on the skin surface. In scalp surgery, the goal is just the opposite. When operating in a hair-bearing area, the object is to minimize the amount of suture in contact with the follicles to prevent hair loss. Therefore, the sutures should run parallel in the fat (so that they don’t cross over and entrap follicles) and be advanced on the surface where any transient suture marks on the skin are irrelevant.
When using small bites very close to the wound edge, sutures tend to get buried within several days after the surgery and become problematic to remove at 1-2 weeks. Poliglecaprone offers a distinct advantage over non-absorbable sutures since they don’t need to be removed.
A more subtle advantage of placing sutures close to the wound edge is that it allows for a greater surface area that can be stretched to close the wound. When large bites are used the elasticity of the skin between the sutures actually pulls the edges away from each other, making approximation more difficult and the wound tension greater.
Recently, Kolasinski described using a running intra-dermal Monocryl suture to close the donor area ((Kolasinski J: Monocryl suture in hair transplantation. Hair Transpl. Forum Int. 2000; 10(3): 77-8. )). This technique has the benefit of avoiding tissue strangulation, but has the disadvantage of a less secure apposition of the wound edges. In addition, it is a more laborious technique. Our limited experience with this suturing method suggests that it may have an advantage over a simple running stitch in very short incisions with no tension, but is inferior for the majority of closures in our practice. Bilateral comparisons need to be made to determine the ideal indications for each technique.
Another advantage of Poliglecaprone suture is the in-vivo duration of its tensile strength. Its initial strength is comparable to that of the very strong, non-absorbable suture polypropylene. At 7 days it maintains 50-60% of its tensile strength and at 14 days (the longest time that non-absorbable sutures are generally left in place) it still has 20-30% of its strength. In situations when there in no undue tension, this permits the wound to be closed without the need for buried sutures. This has the advantage of a shorter operating time and eliminates the possibility that subcutaneous sutures can impinge upon and damage hair follicles.
Because of the excellent tensile strength of Monocryl sutures, we were able to close all of our wounds with 4-0. In non-study patients, with short incisions under no tension, we have occasionally used 5-0 with excellent results. The important point is that using heavier Monocryl sutures (i.e. 2-0 or 3-0) is unnecessary and will result in more inflammation, poorer wound healing and complaints of slow absorption by the patient. As with taking large bites, using a suture heavier than 4-0 will negate many of the benefits of using Monocryl and is strongly discouraged by these authors.
Table 3. Guidelines for Using Monocryl Sutures
- Plan width of donor strip so that there is little or no tension on closure.
- Use tumescent anesthesia to harvest donor strip in mid-fat.
- Use sutures no heavier than 4-0 or 5-0 gauge.
- Use a simple running stitch, advancing each loop on the skin surface.
- Keep needle parallel to, and within 1.5 mm of wound edge.
- Incorporate epidermis and dermis only.
- Use 0.5cm spacing between loops.
In this study, metal staples were chosen for the comparison because they are totally inert, do not cause strangulation of the wound edge, are fast to apply, and have been reported to result in excellent healing6,7. However, our study has shown that they have the disadvantage of being uncomfortable for patients in the post-operative period. In addition, they require a follow-up visit for their removal (which also can be very uncomfortable) and most importantly, result in a wider scar than sutures in most patients when there is even minimal wound tension. In addition, we found that although fast to apply, staples did require some degree of skill to apply properly and required an assistant to hold the wound edges perfectly flush as the staples are applied.
Staples did not appear to hold the wound edges as securely as sutures, so that there was slightly more post-op oozing (this was observed in our practice, but not in the study). In addition, in some patients, neck flexion caused the edges to shift slightly resulting in a slightly perceptible ridge along the suture line (this was never observed with sutures). Finally, staples produced a very distinct linear scar and, even when it was very fine, did not blend in as well with the surrounding hair, as did the scar resulting from Monocryl sutures.
Staples produced a measurably finer scar in two patients in the study. Both of these patients had high density and very loose scalps. This has been consistent with the general experience using staples in our practice. It appears that staples offer a slight, but definite, advantage in these select patients. In our practice, we presently offer the choice of staples to patients who fall into this category of high density and good scalp laxity and who, in addition, are undergoing a relatively small procedure (requiring a donor incision of 14 cm or less).
The best explanation for the generally superior healing with Poliglecaprone sutures over metal staples is the ability to consistently achieve perfect wound edge approximation when sutures are meticulously placed.
The experience in our facilities, where over two thousand patients have had closures using Monocryl sutures, has been that Monocryl has a slightly greater incidence of pruritus than the less than 5% reported in this study. We find that the true incidence is probably on the order of 10-20%. The small n value of this study would likely account for this difference. Post-operative pruritus can be greatly reduced by keeping the suture line occluded with a thin layer of ointment of any kind (we routinely use Bacitracin Ointment) for 2-3 weeks following surgery. It is important to note that, in the current study, excluding tenderness, there was little difference in side effects between the two sides.
A complaint from some patients in our practice, that was not reported by any patients in the study, was persistence of the knots at the ends of the running Monocryl suture. All patients are told pre-operatively that, although the sutures will have lost their strength by three weeks post-op, the knots may persist longer. When the knot persists longer than three weeks it is usually because some hair was incorporated into the knot during the suturing. Since the knot is not subject to hydrolysis by the body, it will sit on the surface of the scalp until it loosens from the hair. The most likely explanation for the difference in the rate of complaints between our general patients and those in the study is the greater attentiveness to pre-operative discussions by patients enrolled in the study and thus the greater awareness that this might occur. After two weeks, any patient complaining of a persistent knot is advised to either return to the office for removal or instructed to simply cut the knot off with fine scissors at home.
In summary, Poliglecaprone 25 (Monocryl) is a very strong synthetic, absorbable, monofilament suture with low tissue reactivity that can be used in hair transplantation to close the donor wound with a single, running cutaneous stitch. If specific surgical techniques are followed, suturing with Monocryl can produce a fine surgical scar superior to metal staples and can result in a more comfortable post-operative experience for the patient.
Acknowledgement
This work was performed at the New Hair Institute, 125 East 63rd St., New York, New York, and 2150 Center Ave., Fort Lee, New Jersey.



