In this Case Study, we will change the format a bit and have each question relate to a different patient.
Patient #1
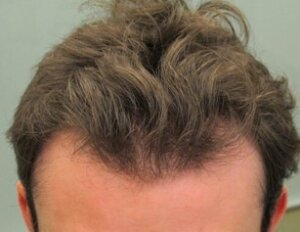 Your first patient of the day is a 21-year-old male seeking evaluation for rapid hair loss. He and his parents – who were present at the consult – are requesting a hair transplant. He is complaining that he has more hair in the shower, has less hair volume, and is “beginning to look like my father.” He is hesitant to use medications, as he is concerned that “he will need to be on these medications forever.” On physical exam, he has markedly receded temples and some thinning in his crown consistent with a Norwood Class 3V pattern. His older brother, who has very little hair loss, has already started using finasteride. His father had hair on the back and sides of his scalp, but none on the top.
Your first patient of the day is a 21-year-old male seeking evaluation for rapid hair loss. He and his parents – who were present at the consult – are requesting a hair transplant. He is complaining that he has more hair in the shower, has less hair volume, and is “beginning to look like my father.” He is hesitant to use medications, as he is concerned that “he will need to be on these medications forever.” On physical exam, he has markedly receded temples and some thinning in his crown consistent with a Norwood Class 3V pattern. His older brother, who has very little hair loss, has already started using finasteride. His father had hair on the back and sides of his scalp, but none on the top.
Question 1: What should you do next?
- Discuss medical therapy with finasteride and minoxidil in spite of the patient’s hesitancy to use them.
- Discuss FUE and FUT hair transplant options.
- Use densitometry to check for miniaturization in the mid-scalp and in the back of his scalp.
- B & C
- A & C
Answer E. It is quite common for people to be hesitant to use finasteride. If you feel that it is the best treatment, it is in the patient’s best interest to present a strong case to use this medication. The common pushback of “I will need to be on these medications forever” is easy to work around. Simply point out that almost all medications only work when you are using them and that although finasteride is the best option now, in the future many other options are likely to be available.
Although minoxidil is also effective, it is far less so than finasteride and the combination of finasteride and minoxidil is the best treatment for early hair loss in a young person.
Densitometry is an essential part of the hair loss evaluation and gives important information about the extent of the hair loss that is not readily ascertained on gross inspection.
A hair transplant should not be considered in a patient under the age of 25, especially for those who have not yet had treatment with medication. Extensive hair loss at this age would be another concern. As a general rule, the earlier the hair loss begins, the worse the prognosis. Since a hair transplant depends upon an adequate donor supply to cover a limited area of hair loss. The supply/demand ratio does not work in a patient with a risk of extensive loss. It is also important to point out that since a hair transplant does not prevent further loss, it should never be used as a preventive treatment.
Patient #2
 Your next patient is a 23-year-old male who has a patch of hair loss on his left temple that has been present “as long as I can remember.” His mother had Hashimoto’s thyroiditis.
Your next patient is a 23-year-old male who has a patch of hair loss on his left temple that has been present “as long as I can remember.” His mother had Hashimoto’s thyroiditis.
Question 2: What should you do next?
- Perform thyroid function tests
- Look for other suspicious lesions
- Begin topical minoxidil and retinoic acid
- Discuss FUE and FUT hair transplant options
- All the above
- A & C
- B & D
Answer G. The first answer is a red herring. This lesion has the typical clinical appearance of Triangular Alopecia. It has the typical shape and location of this condition. The lesion is smooth, but not scarred, and the border has vellus hairs. There are no exclamation point hairs seen in alopecia areata. The history of a congenital process is the clincher. A biopsy, although confirmatory, is not generally needed.
The second answer is also a bit of a red herring. Since this is not alopecia areata, you would not expect to see other lesions on the body. However, triangular alopecia is often bilateral and lesions can rarely occur on the nape of the neck.
The treatment is surgical and either FUT or FUE hair transplant procedures can be considered. Topical therapy has no role in the treatment of this condition.
Patient #3
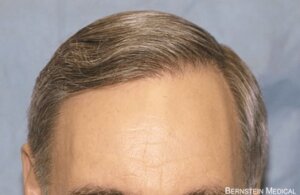
 Your next patient is a 58-year-old woman complaining of a slowly receding frontal hairline. She finished menopause at age 52. Her father and maternal brother had extensive hair loss from an early age. She has been using topical minoxidil for the past year.
Your next patient is a 58-year-old woman complaining of a slowly receding frontal hairline. She finished menopause at age 52. Her father and maternal brother had extensive hair loss from an early age. She has been using topical minoxidil for the past year.
Question 3: What should you do next?
- Perform a scalp biopsy
- Begin medical therapy with oral minoxidil and spironolactone
- Consider a hair transplant and explain to the patient that two procedures may be necessary
- Begin treatment with corticosteroids
- B & C
- A & D
Answer F. The irregular frontal hairline with erythema, scattered terminal hairs, and the lack of significant miniaturization, strongly suggests a diagnosis of frontal fibrosing alopecia. On closer inspection there is perifollicular erythema and scale and areas completely devoid of hair follicles.
The next step is to perform a scalp biopsy to confirm the diagnosis, but in this case the clinical presentation is so characteristic that the initiation of therapy is reasonable. Initial treatment generally involves some form of corticosteroids (either topical or intralesional) often in combination with another anti-inflammatory agent.
Patient #4
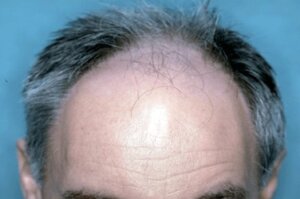 The last patient is a 55-year-old-male complaining of progressive hair loss over the past 15 years. He claims that his maternal uncle has a similar pattern, but his father, at age 78, still has “a full head of hair.” On physical examination, he has minimal hair loss in the crown and you decide that he has a Norwood 5A pattern of hair loss.
The last patient is a 55-year-old-male complaining of progressive hair loss over the past 15 years. He claims that his maternal uncle has a similar pattern, but his father, at age 78, still has “a full head of hair.” On physical examination, he has minimal hair loss in the crown and you decide that he has a Norwood 5A pattern of hair loss.
Question 4: What should you do next?
- Perform a scalp biopsy
- Begin medical therapy with finasteride and minoxidil
- Discuss hair transplant surgery
- A & B
- B & C