The Operating Room
Follicular Unit Transplantation is typically performed in an out-patient, office setting. The guidelines of care for office surgical facilities delineated by the American Academy of Dermatology should be reviewed before setting up facilities. 39,40 Though major complications during surgical hair restoration occur only rarely, protocols should be in place to handle emergencies such as hypersensitivity reactions/anaphylaxis, stroke, seizures, arrhythmias, acute myocardial infarction and hypertensive crisis. At a minimum, specific arrangements should be made with a local Emergency Medical Services (EMS) facility to take care of distressed patients.41
The medical staff should be comfortable dealing with problems such as bleeding, syncope (with or without petit mal episodes) and anxiety reactions. The medical staff should be certified in cardiopulmonary resuscitation and at least some in advanced cardiac life support. The amount of in-office emergency equipment will depend on staff capabilities and training and proximity to an EMS unit. Basic equipment includes portable oxygen, an automated defribulator, IV setup and oral or nasopharyngeal airway.41
Because of the scalp’s abundant vascular supply and relative resistance to infection, it is common practice for hair transplant surgeons’ technique to be aseptic, rather than sterile. And since the scalp is not usually shaved and prepped, strict sterile technique is not practical. However, at least until the donor area is sutured closed, a sterile environment should be maintained. This issue is discussed in greater detail by Sebben and Davis.42,43
The single most important instrument for FUT is the dissecting stereo-microscope,9,44 which is available with either a binocular view or with LCD screen. Each member of the surgical hair restoration team performing the dissection should have one. Experienced teams generally require one staff member per 500 to 750 grafts (for graft dissection and placing), so that a typical 2000-graft hair transplant surgery would necessitate three to four staff members in addition to the physician, though this will vary tremendously among practices. Less-experienced teams may require more people. The staff’s other responsibilities as well as possible absenteeism must also be taken into account.
Regular operating-room tables are generally inadequate. Rather, the tables must be contoured and provide some lumbar support when hair transplantation patients are sitting. They also need to be low to the ground, with the seat not more than 56 cm from the floor, so the staff can work comfortably around the head while the patient is seated.
Equally important are comfortable working areas for the staff. Dissecting tables with a bull nose, rather than squared edge, are easier on their arms, and adjustable seating saves them from bending over to look into the microscopes (Fig. 34.5). The long duration of the hair restoration surgery makes meticulous attention to ergonomic issues all the more crucial.45 Bright fluorescent ceiling lighting is preferable to surgical OR lights because it generates less heat. We use high-intensity surgical lights only for working on the donor area, as they can be angled to illuminate the posterior scalp of the seated hair transplant patient.46
The Petri dishes containing grafts pending placement should be kept on a stable, wall-mounted surface to keep them from being inadvertently knocked over (Fig. 34.6). The typical operating room Mayo stand is not stable enough.47 Normal saline is the most frequently used holding solution for grafts, but we prefer the more physiologic Lactated Ringer’s. Limmer has shown a high survival rate for grafts kept in chilled saline up to eight hours.48 More exotic solutions with potential graft-sustaining properties have been developed, but they are not widely used.49,50
 Fig. 34.5 Dissecting stereo-microscopes on cutting table.
Fig. 34.5 Dissecting stereo-microscopes on cutting table. Fig. 34.6 Wall-mounted placing stand for ice blocks, grafts and instruments.47
Fig. 34.6 Wall-mounted placing stand for ice blocks, grafts and instruments.47Grafts should be refrigerated most of the time they are outside the body. Approximately one hour prior to placement, we remove a portion of the grafts from refrigeration and put them into Petri dishes that are resting on ice packs that maintain the Ringer’s solution at 59º C. This is set on a wall-mounted stand conveniently located at the head of the operating chair.
It is preferable to have all the dissection performed in the operating room. In addition, a small refrigerator used solely for graft storage should be located in each room. Performing all the dissection and storing the grafts in the same room eliminates the risk of inadvertently placing grafts in the wrong patient. Although obvious, this is particularly important in a busy practice where more than one person is being operated on per day. The minimum room size for a hair restoration doctor and five staff members to work comfortably is approximately 15.5 sq meters.
In advance of the hair transplantation procedure, it is helpful to set up complete surgical trays, including the local anesthetic mixtures predrawn into syringes. This serves a number of purposes: it makes it easier to keep track of how much anesthetic is used in each part of the hair transplant surgery, ensures that safe dose limits are not exceeded51 and minimizes the risk of needle-stick injury, since the preparation takes place before the OR begins to bustle.
Local anesthesia is administered with a ring-block consisting of lidocaine, bupivacaine and epinephrine buffered with sodium bicarbonate. Lidocaine, the major component, is used for its safety and quick onset. Bupivacaine is added to increase the duration of anesthesia, but in smaller quantities to limit its potential cardiac toxicity.52 Epinephrine increases the anesthetic duration while decreasing its toxicity and providing some hemostasis, though its vasoconstrictive action is relatively short-lived. Bicarbonate is added to bring the acidic pH of the epinephrine containing solution closer to 7.4, lessening its sting.53 This is particularly useful for injections at the hairline, where the scalp tends to be most sensitive. Though mentioned elsewhere in this text, it is worth repeating that the combined use of epinephrine and broad ?-blockers (e.g. propranolol) can result in potentially life-threatening reactions.54
The anesthetic solution used for a typical 2000-graft hair restoration session is listed in Table 34.8. The anesthetic is drawn into 13 5-cc syringes then fitted with 27-g needles. The tumescent mixture consists of 3 10-cc syringes with 25-g needles. These quantities are preprinted on the operative report and circled as each syringe is used. If patients require additional anesthesia, they are reevaluated and then the medication drawn up and dose recorded.
Techniques
On arriving at the office, patients sign the consent form (which had been given to them well in advance). The surgical plan is reviewed and any last-minute questions answered. Next, density is checked to confirm the measurement taken at the initial consultation; if the number differs or it appears that density varies in the donor area, multiple measurements are taken. Scalp laxity is also reassessed and recorded on the operative report.
Patients proceed to change into a cotton surgical gown and have their picture taken with a digital camera against a light-blue background. Then the hairline and other important landmarks, such as the vertex transition point and crown swirl, are marked in Gentian violet and shown to the patient using two mirrors. If the patient approves of the hairline design, additional pictures are taken, this time of the marked scalp, usually from the front and aerial views. Three-quarter and close-up photos are sometimes taken to illustrate particular cosmetic issues. Occasionally pictures will be taken during and after the hair transplant for teaching purposes. All photos are kept as part of patients’ permanent medical record.
Typical patients are premedicated with diazepam 15 mg PO, Dicloxacillin 1000 mg PO (with a second dose of 500 mg six hours into the hair transplantation procedure) and an intramuscular injection of methylprednisolone 80 mg, i.e. 40 mg in each arm.
Donor Harvest
In preparation for the donor harvest, patients are seated upright on the operating table. The hair in the donor area–that covering the donor strip plus the 0.5 cm beyond its perimeter–is then cut to 1-2 mm using electric clippers (the extra 0.5 cm to facilitate suturing). The trimmings are thoroughly vacuumed away and the hair above the strip is held back with tape, fully exposing the donor area. A gauze headband is placed around the patients’ head just below the clipped area and sterile drapes are taped to the headband.
In the first surgical hair restoration session, in a patient with average scalp laxity, we generally harvest a donor strip that is 1 cm wide. In calculating the length, we use the general rule of 100 follicular units per cm2.6 For example, if 1500 follicular unit grafts are planned, the strip would measure 18 cm in length (15 cm + 3 cm for tapering). Africans and occasionally Asians will have a lower follicular unit density and a strip of this dimension will yield a lower number of follicular unit grafts. However, the length should not be increased; rather the session should be planned using fewer grafts.8
Local Anesthesia
A ring-block is established using a lidocaine/marcaine/adrenaline anesthetic mixture. The anesthetic solution is injected into the deep subcutaneous fat layer approximately 1 cm below the lower portion of the clipped area and extending several centimeters past it on either side.
Approximately 0.75 cc of anesthesia are used per centimeter of donor area, so that a 25-cm-long incision would require slightly less than 20 cc of anesthetic solution. It is important to avoid injecting into the muscle, as epinephrine will cause vasodilatation (due to the action on ß2-receptors), quickly dissipating the local effects of the anesthetic and increasing its toxicity.56
The ring-block takes approximately 15 minutes to induce anesthesia. As soon as the donor-area skin becomes numb, tumescent anesthesia is administered by injecting larger quantities of a more dilute epinephrine solution into the mid-fat to make the area firm. The tumescence serves six purposes: 1) to widen the distance from the follicles residing in the upper fat to the nerves and larger blood vessels lying just above the fascia, 2) to increase the rigidity of the donor area, 3) to decrease follicular transection, 4) to decrease bleeding, 5) to produce more uniform anesthesia and 6) to reduce the amount of anesthetic required.
Tumescence can be achieved using a dilute solution of epinephrine (adrenaline) and lidocaine in somewhat higher concentrations than used in liposuction surgery, as this will provide additional anesthesia that is particularly important in repeat hair transplants or for patients with significant donor scaring.57 In situations where there is scarring, direct cutaneous innervation to the donor area from the occipital branches can be blocked so that innervation to the donor area arrives in a rostral-caudal direction rendering inferiorly placed ring-block anesthesia ineffective. At times, when there is an excessive amount of donor scarring, even the tumescence is inadequate and the initial ring-block mixture must be injected above or directly into the scarred area to make it numb.
Table 34.8 Anesthetic Mixture
Follicular Unit Extraction
Follicular Unit Extraction (FUE)2 is a conceptually simple hair restoration procedure, where individual follicular units are harvested through a small circular incision created by a trephine or similar instrument. The punch cuts into the reticular dermis and the remainder of the follicular unit is literally extracted from the scalp. The advantage of this procedure is that it obviates the need for a linear incision. Difficulties lie in the intrinsic variability of each patient with respect to the ease of extraction, the increased risk of follicular transection compared to other hair transplantation techniques, and the organizational limitations of not being able to have multiple persons (more than two) working in parallel, as with microscopic dissection.
Follicular Unit Extraction (FUE) is appropriate for hair transplant patients who have limited hair loss and who want to wear their hair so short that a linear donor scar might become visible. The procedure is also useful in patients who have healed poorly, or who have a very tight scalp. The most important application of this technique, however, is to camouflage a linear donor scar from a prior hair transplant procedure.2
FUE’s main limitation is that it is less efficient in harvesting hair than follicular unit transplantation performed with strip harvesting. In FUT, all the hair from the optimal (central) part of the donor region can be removed and transplanted, and the resulting defect is sewn closed. In contrast, the FUE defects remain open to heal by secondary intention with significant amounts of intervening hair left behind and, therefore, a much larger region must be accessed to harvest the necessary amount of donor hair.
With Follicular Unit Extraction, the secondary-intention healing causes microscopic fibrotic changes in the donor area, distorting adjacent follicular units and making subsequent sessions more difficult. As mentioned, transection during the harvest is appreciably greater than stereo-microscopically controlled FUT. Taken together, these factors significantly limit the total amount of hair that can be accessed through FUE rendering it a less robust procedure than Follicular Unit Transplantation. In a procedure where a finite donor supply is the main constraint, inefficient use of donor tissue poses a significant problem. Table 34.9 summarizes the pros and cons of this follicular unit extraction.
The ability to perform follicular unit extraction with minimal transection varies significantly among patients. Because of this, a test measuring the ease of extraction (the FOX Test)2 should be performed prior to recommending the hair restoration procedure. Patients undergoing follicular unit hair transplantation should also be tested for follicular unit extraction at the time of surgery, in case the latter procedure is needed (or desired) at a future date. It is encouraging that follicular unit extraction techniques continue to improve.
Table 34.9 The Pros and Cons of Follicular Unit Extraction
Pro
• No linear scar
• Useful when the patient wants (or needs) to wear the hair on the back and sides very short
• Useful when only small numbers of grafts are needed (e.g. limited hair loss, a small touch-up hair transplant procedure)
• Provides an alternative when the scalp is too tight for a primary closure or when the patient heals with widened scars
• Ideal for camouflaging donor scars that cannot be excised
• Makes it possible to harvest non-scalp hair (e.g. beard or body hair)
Con
• Requires multiple sessions to equal the size of a single FUT procedure
• The number of grafts that can be obtained is limited to 400 to 600 at a time
• Takes longer to perform and is more expensive than FUT
• Risks the eventual loss of transplanted grafts by harvesting from outside the “sweet spot” of permanent hair in the donor zone
• After large numbers of graft are harvested, fine stippled scars may become visible due to thinning of donor area
• Scarring and distortion of follicles may make further harvesting by follicular unit extraction difficult
• Maximum possible yield markedly lower than with FUT
Strip Excision
The ideal position for the donor incision is in the mid-portion of the permanent zone lying at the level of the external occipital protuberance. A 1-cm-wide donor strip is excised using two parallel blades set 1.2 cm apart. (The extra 2 mm accounts for the skin stretched from the tumescence.) A convenient harvesting device is the Rassman handle that is loaded with two #10 blades. The handle holds the blades at an angle of 30º, making them parallel to the emergent hair.1 The handle should hold the blades in a preangled position; otherwise, in following the angle of the hair, the hair restoration doctor may cut superficially with the upper blade while too deep into the scalp with the lower (Fig. 34.7). Once the main parallel portion of the incision is complete, a single scalpel blade is used to taper the ends into an ellipse. In general, the length of each tapered end should measure at least 1.5 times the width of the strip so that the ends lie flat (Fig. 34.8).
Alternatively, the entire excision can be performed with a long free-hand ellipse after the skin is marked.9 This allows the angle of the blade to be adjusted as each edge is cut. On the other hand, this hair transplant surgery technique makes it harder to keep the width uniform, which is necessary for predictable graft yields. Cutting the second edge also becomes more difficult because the rigidity of the tumescence is lost. The first incision renders the second wound edge mobile and there is more distortion of the wound edge and hair follicles due to the relative elasticity of the dermis compared to the epidermis and fat.
 Fig. 34.7 Donor-strip harvesting using two parallel blades on a Rassman handle pre-angled at 30º to allow both blades to lie flush against the scalp.
Fig. 34.7 Donor-strip harvesting using two parallel blades on a Rassman handle pre-angled at 30º to allow both blades to lie flush against the scalp. Fig. 34.8 Dissection at the tapered corner of the strip in a mid-subcutaneous plane, just below the follicles.
Fig. 34.8 Dissection at the tapered corner of the strip in a mid-subcutaneous plane, just below the follicles.Donor Closure
Once the strip is removed it is immediately placed into a chilled Ringer’s lactate solution. The donor wound is sutured with a running 5-0 suture made of poliglecaprone 25,58 although a wide variety of suture materials and techniques are available.59,60 Absorbable sutures can be placed very close to the wound edge, so close that they are quickly buried after the hair transplantation procedure making removal difficult. Placing sutures close to the wound edge minimizes entrapment of follicles and avoids strangulation if there is significant post-op edema. To further limit damage to follicles, the sutures should be placed approximately 4.5 mm apart and the suture should be advanced on the surface, rather than under the skin (as in traditional hair restoration surgery), as this will minimize the amount of suture in contact with the follicles (Fig. 34.9).
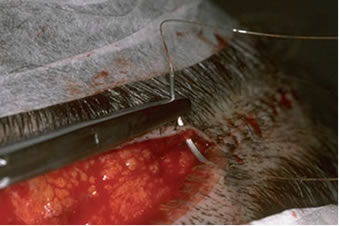 Fig. 34.9 Suturing the donor area using absorbable sutures. Note the needle track is parallel and very close to the wound edges.58
Fig. 34.9 Suturing the donor area using absorbable sutures. Note the needle track is parallel and very close to the wound edges.58 Fig. 34.10 Schematic of the suturing technique recommended for sewing the donor scalp. The spacing between loops is from 4.5 to 5 mm58
Fig. 34.10 Schematic of the suturing technique recommended for sewing the donor scalp. The spacing between loops is from 4.5 to 5 mm58The needle should be passed through the full thickness of the dermis and exit the wound edge just below it (at the level of the bulbs) without incorporating any significant amount of subcutaneous tissue. The needle track must be kept parallel to, and within 1.5 mm of the wound edge (Fig. 34.10). Particular attention should be paid to placing the needle parallel to the upper wound edge where the angle is very acute. Basic guidelines for using poliglecaprone 25 (Monocryl) sutures can be found in Table 34.10.
Table 34.10 Guidelines for Using Poliglecaprone 25 Sutures
• Plan width of donor strip so that there is little or no tension on closure.
• Use tumescent anesthesia to harvest donor strip in mid-fat.
• Use sutures no heavier than 4-0 or 5-0 gauge.
• Use a simple running stitch, advancing each loop on the skin surface.
• Keep needle parallel to, and within 1.5 mm of, wound edge.
• Incorporate epidermis and dermis only.
• Use 4.5 mm spacing between loops.
If staples are used to close the wound edges, it is important to be certain that the wound edges are flush before the staples are applied. The edges can be approximated by grasping the lower edge with a skin hook and using rat-toothed forceps to hold and slightly evert the upper edge (this requires the help of an assistant). The staples should then be placed approximately 0.6 cm apart (Fig. 34.11). Staples have virtually no tissue reactivity, but they make flush apposition of wound edges difficult and can be uncomfortable and painful to remove. In the balance we prefer absorbable sutures, though staples may be better for some hair transplant patients with high density and very loose scalps.58
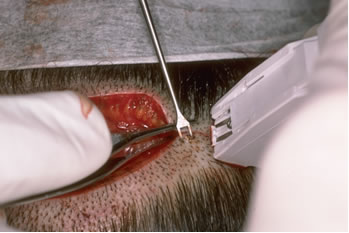 Fig. 34.11 Stapling technique illustrating very controlled apposition of wound edges, using skin hooks for the lower edge and forceps to evert the upper.58
Fig. 34.11 Stapling technique illustrating very controlled apposition of wound edges, using skin hooks for the lower edge and forceps to evert the upper.58Graft Dissection
Once the donor strip is removed, it is immediately placed into Lactated Ringer’s solution and passed to the head member of the surgical team stationed at a stereo-microscope (Fig. 34.12). The strip dimensions are measured and recorded. The next step is performed under strict stereo-microscopic control in a process called “slivering.”10,35
 Fig. 34.12 Close-up view of a donor strip showing the natural hair groupings at the surface, slightly curved path of the hair through the dermis and random distribution of bulbs in the fat. It is this unique anatomy that makes stereo-microscopic dissection essential in preventing follicular transection.
Fig. 34.12 Close-up view of a donor strip showing the natural hair groupings at the surface, slightly curved path of the hair through the dermis and random distribution of bulbs in the fat. It is this unique anatomy that makes stereo-microscopic dissection essential in preventing follicular transection.In one method of slivering, the donor strip is placed on its side, on a wooden tongue-depressor blade (soaked in Ringer’s) with the hair pointing away from the dissector and the convex surface of the strip facing upward. For a right-handed person performing dissection, the left end of the strip is held with rat-toothed forceps in the dissector’s left hand. An assistant applies tension to the strip, holding it a few centimeters away from the area being cut with rat-toothed forceps held in the right hand. Using a Personna #10 blade on a #3 blade handle held in the right hand, the dissector begins to cut the strip into 2-2.5 mm wide sections, by guiding the blade between follicular units using a one-directional fillet-like movement from the epidermal side to the subcutaneous surface. A back-and-forth sawing motion should be avoided as it will destroy follicles (Fig. 34.13, 34.14). The pieces generated are then passed along to the other members of the surgical hair restoration team who complete the dissection. In the last step, the individual pieces are placed on their sides, stabilized with straight jeweler’s forceps, and then dissected under the stereomicroscope with a scalpel into individual follicular units of one to four-hairs (Figs 34.15, 34.16).
 Fig. 34.13 “Slivering” the donor strip into sections.
Fig. 34.13 “Slivering” the donor strip into sections.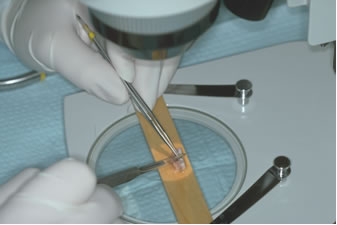 Fig. 34.14 Stereo-microscopic dissection of one section into smaller pieces.
Fig. 34.14 Stereo-microscopic dissection of one section into smaller pieces.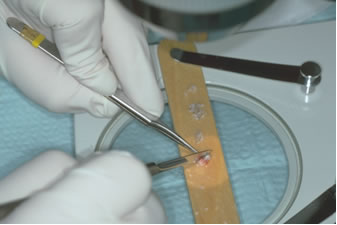 Fig. 34.15 The final step of the dissection: generating individual follicular units.
Fig. 34.15 The final step of the dissection: generating individual follicular units.Next, the units are sorted according to the number of hairs they contain into separate Petri dishes held on ice blocks and filled with Ringer’s lactate (Fig. 34.17). When a substantial number of grafts (several hundred) have been dissected, they are put into more secure plastic specimen containers and refrigerated.
 Fig. 34.16 Dissected one-, two-, three- and four-hair follicular units.
Fig. 34.16 Dissected one-, two-, three- and four-hair follicular units.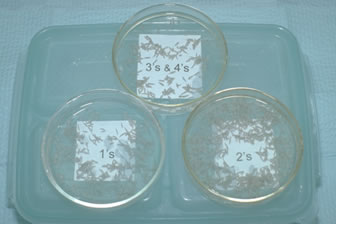 Fig. 34.17 Petri dishes with one- to four-hair follicular units immersed in Ringer’s lactate.
Fig. 34.17 Petri dishes with one- to four-hair follicular units immersed in Ringer’s lactate.An alternate slivering method involves dissecting the donor strip into slivers as wide as one follicular unit, approximately 1 mm. The units are then isolated from the very thin strip. The key to either hair transplantation method is that every step is performed under stereo-microscopic control, which keeps the units intact and avoids follicular transection. It is also vital that all the pieces of the strip remain in chilled Ringer’s lactate except when they are being cut. While under the microscope, they should be kept well-hydrated using 10-ml syringes containing Ringer’s lactate, kept by each cutting surface.
Recipient Sites
The way recipient sites are prepared determines the critical aesthetic factors of the hair transplant: the angle at which the new hair grows, its distribution, its density and how natural the hair will look as it emerges from the scalp. A thorough discussion of site creation is beyond the scope of this chapter, but the four basic elements will be briefly reviewed. These are recipient site size, hair direction, site density and graft distribution, and they are covered in greater detail in Bernstein and Rassman.8
Recipient Sites
The sites should provide a snug fit for the graft: just large enough to accommodate a follicular unit, but not so small that insertion is difficult or traumatic.1 Numerous instruments have been developed to create recipient sites. The main aspect to consider in choosing one is its diameter.61 Although there are many viable options, the following are suitable for most hair restoration procedures:
• a 19- or 20-gauge hypodermic needle for one-hair and thin two-hair follicular unit grafts
• an 18-gauge needle for thick two-hair and all three- and four-hair follicular unit grafts
These needles can be fitted on 3-ml syringes for ease of use, obviating expensive handles. Some hair transplant doctors advocate smaller recipient sites, but this may require dividing four-hair follicular units, a technique that this author does not recommend.35 For very fine hair, or in special situations like transplanting eyebrows, a 20-gauge (or finer) needle can be used.
Most instruments used to make sites create tiny slits as they cut through the skin, and these slits can have either a coronal (horizontal) or sagittal (vertical) orientation. The purported advantages of coronal incisions are: a more natural appearance (since the original orientation of most follicular units seems to be coronal), a fuller look and less tendency of the growing hair to elevate in the vertical plane. The purported advantages of a sagittal orientation are: greater visibility of sites, ease of graft placement, less trauma to existing hair, less damage to collagen and the underlying vasculature and less lateral (radial) splay of hair.
Hair Direction
Hair should be placed into the scalp at the angle it originally grew in, not in the direction that it is to be groomed. In general, hair anterior to the vertex transition point should point forward, with the angle becoming more acute as it reaches the anterior hairline, where it is essentially horizontal to the ground (regardless of the slope of the forehead). The direction of hair in the frontal hairline always points forward, rather than growing radially, and only deviates significantly from this as it approaches the temples (Fig. 34.18).8
 Fig. 34.18 Normal hair direction: A) top view, B) side view.8
Fig. 34.18 Normal hair direction: A) top view, B) side view.8Recipient Site Density
The average non-balding scalp has 100 follicular units per cm2. Approximately 50% may be lost before there is any noticeable thinning. It would be wasteful, therefore, for more than 50% to be replaced–especially since hair transplants are always performed in the face of diminished total hair volume. We generally recommend transplanting up to 25 follicular units per cm2 into the frontal area of a balding scalp. If the larger three- and four-hair units are placed in select areas, more than 25% of the initial density can be achieved in one pass. With two procedures the ideal transplant density can be achieved in many patients.8
Some physicians advocate a “one-pass” hair restoration procedure to achieve the final density.35 Although this may be appropriate for some patients, the increased incidence of graft popping and desiccation, insertion injury and possible vascular compromise may lead to poor growth. For very bald patients, very dense packing does not allow coverage of an entire bald area. Moreover, hair transplants of more than 2500-3000 follicular units often necessitate that the grafts be out of the body so long that their survival may be diminished. It is this author’s view that covering the entire bald area and then increasing density in a subsequent session is a better goal for most patients as this avoids the risks of very dense packing.
Distribution
For simplicity, the area of the scalp subject to androgenetic change can be divided into three regions: 1) the frontal region that includes the frontal hairline, 2) the top or mid-scalp and 3) the vertex or crown. The vertex transition point separates the top of the scalp from the crown (Fig. 34.19).34 Since most social interaction takes place face to face and people generally view themselves from the front, the overall impact of the hair transplantation is defined by the position of the frontal hairline and density of the frontal region of the scalp.
 Fig. 34.19 Regions of the scalp.
Fig. 34.19 Regions of the scalp.For most hair transplant patients who are moderately to extensively bald, or destined to be, the limitations of the donor supply make restoring the entire bald scalp to ideal density impossible. Consequently, creating the greatest density in the front part of the scalp produces the best cosmetic result. This “forward weighting” can be accomplished by putting recipient sites closer together, placing larger follicular units (i.e. those with three and four hairs) in those sites, or by doing both.
In general, recipient site density should be the highest in the front part of the scalp and gradually tapered toward the crown. In contrast, the largest follicular units should be placed in the forelock region of the scalp. This overlapping distribution of sites and follicular unit grafts may be visualized in Figure 34.20. It is explained in greater detail in the paper, The Aesthetics of Follicular Transplantation.8 The pattern serves two functions: it creates a natural central-forelock density without the need for spacing sites closer towards the mid-scalp (where the blood supply can most easily be compromised) and ensures the most natural look by placing the larger follicular units in a forward-central position, but away from the frontal hairline. Density in the forelock area brings about a “patterned look” and avoids the diffuse thinning that often results when small grafts are evenly distributed over the scalp.
 Fig. 34.20 Schematic of “forward weighting,” achieved by close placement of recipient sites dark grey area), and central density, accomplished by placing larger follicular units in the forelock area (dark brown oval).
Fig. 34.20 Schematic of “forward weighting,” achieved by close placement of recipient sites dark grey area), and central density, accomplished by placing larger follicular units in the forelock area (dark brown oval).Practically every hair restoration patient has enough donor hair to provide at least light coverage extending to the vertex transition point. This is a natural stopping point since, even if the crown continues to enlarge, transplants performed to this point will still look natural without additional hair transplant surgery. Transplants should be extended past the vertex transition point into the crown only when there is adequate hair to create a swirl and follow the hair loss if the balding progresses. The indications for transplanting the crown are discussed in detail in Follicular Transplantation: Patient Evaluation and Surgical Planning.7
The distribution of grafts in the first transplant session should, in general, be symmetric. However, once the first hair transplant has had a chance to grow and the patient is willing to commit to styling his hair in a specific pattern, “side weighting” should be considered. This is accomplished either by placing a greater proportion of the grafts on the parted side of the scalp, using larger follicular units on that side, or doing both. It results in increased fullness when one’s hair is combed to the side. In situations where there is a great imbalance in the supply/demand ratio, such as after scalp reductions or old plug procedures, a more exaggerated form of “side weighting” should be considered. In this case the follicular unit grafts are concentrated on the front and part side of the scalp but widely scattered in the top and back.8 (Fig. 34.21)
 Fig. 34.21 Left: Schematic view of left to right “side weighting.” Right: Extreme side weighting employed when the donor supply is severely diminished.
Fig. 34.21 Left: Schematic view of left to right “side weighting.” Right: Extreme side weighting employed when the donor supply is severely diminished.The number of follicular unit grafts required in the first and subsequent transplant sessions, with and without crown coverage, can be found in Tables 34.4 and 34.5.
When the follicular units are completely dissected and grouped in Petri dishes, they are placed at the head of the operating table on ice blocks. Graft placement, carried out in a front-to-back pattern, begins at the frontal hairline with one-hair follicular units. In a typical hair transplant, approximately 250 one-hair units are used for the leading edge of the frontal hairline, immediately followed by two-hair grafts. Three- to four-hair units are concentrated in the forelock area, (Fig. 34.22) while toward the back and sides the pattern is reversed so that the three- and four-hair units are always central to the one- and two-hair units.
 Fig. 34.22 Staff using loop magnification and curved jeweler’s forceps to place follicular unit grafts into pre-made recipient sites.
Fig. 34.22 Staff using loop magnification and curved jeweler’s forceps to place follicular unit grafts into pre-made recipient sites.Approximately 20-30 grafts are transferred at one time from the dish to the index finger, held on the finger in a droplet of Ringer’s solution. The grafts are inserted using curved jeweler’s forceps. Each graft should be carefully grasped by the fat at its bottom or at its edge, not at the germinative center. In the two-hand technique, gauze, held between the free fingers of the hand holding the grafts, is used to keep the partially inserted grafts in place as the forceps are repositioned higher along the length of the graft, to facilitate the last phase of insertion.
In an alternative method, termed “stick and place,” the grafts are inserted at the same time that the recipient sites are made.35 In this hair transplantation technique, the needle that is used to make the recipient hole can also serves as a “shoehorn” to help guide the graft into the site. The advantage of this method is that it eliminates the possibility that sites may be left unfilled or that two grafts may be placed into one site (piggybacking). It also moves the surgery along faster since the staff doesn’t need to wait for the hair restoration doctor to make the sites and they don’t need to search for the ones that are empty.
On the other hand, there is more bleeding when sites are made concomitantly with graft placement (decreasing visibility) and there is an increased risk of the grafts popping and then drying out on the surface of the scalp. In addition, the staff must make judgments regarding the angling and distribution of the sites they are creating at a time when they must also be focusing on the technical aspects of graft insertion. This leaves many of the aesthetic decisions in the hands of the technicians, who are actively engaged in stick and place, rather than with the physician who could take a more strategic view of the hair transplant surgery.
Patient Disposition
After graft insertion is complete, the scalp is cleaned with distilled water, bacitracin zinc ointment is applied to the sutures and a head-band type pressure dressing is placed over the donor area. The transplanted area is covered with a hair transplant surgeon’s cap. Prior to leaving, patients are given verbal and printed post-op instructions, a neck pillow and medications for sleep, pain and hiccups. Patients leave the office wearing a bandana covering the cap and the headband. It is worth stressing that patients given sedatives or pain medication do not drive after hair restoration surgery.
Table 34.11 Medications Commonly Used in Hair Transplantation