
Robert M. Bernstein, M.D.,* William R. Rassman, M.D.,** Wojciech Szaniawski, M.D.,*** Alan J. Halperin, M.D.****
* Assistant Clinical Professor of Dermatology, College of Physicians and Surgeons, Columbia University, New York, NY.
** New Hair Institute, 9911 West Pico Blvd., Suite 301, Los Angeles, CA 90035.
*** Dermatopathology Associates of New York
**** Dermatopathology Associates of New York
International Journal of Aesthetic and Restorative Surgery 1995; 3(2):119-132.
ABSTRACT
Follicular Transplantation is a method of hair restoration surgery which recognizes the follicular unit as the basic element of tissue to be moved in the transplant. The anatomic and physiologic basis of this procedure, as well as its potential advantages, are discussed. We then describe in detail how follicular implants may be used in extensive quantities for the treatment of androgenetic alopecia. Key Words: Hair Transplantation, Hair Restoration Surgery, Follicular Transplantation, Follicular Unit, Androgenetic Alopecia, Hair Transplant Surgeon
INTRODUCTION
Follicular Transplantation is the logical end point of over 30 years of evolution in hair restoration surgery beginning with the traditional large plugs and culminating in the movement of one, two and three hair units, which mirror the way hair grows in nature. The key to follicular transplantation is to identify the patient’s natural hair groupings, dissect the follicular units from the surrounding skin, and place these units in the recipient site in a density and distribution appropriate for a mature individual. The critical elements of follicular transplantation are an accurate estimation of the donor supply of hair, meticulous dissection of the follicular units, careful design of the recipient area to maximize the cosmetic impact of the hair transplant, the use of large numbers of implants in fewer rather than more sessions, a long-term master plan that accounts for the progression of the male pattern alopecia, and realistic expectations on the part of the patient.
FOLLICULAR UNITS
The concept of follicular transplantation is based upon the observation that, in general, hair does not grow singly, but with the exception of the hairline, emerges from the scalp in groups called follicular units. Histologically, these units are comprised of 1 to 4 terminal and 1 to 2 vellus hairs that form a distinct group bounded by a circumferential band of adventitial collagen, the perifolliculum ((Headington JT: Transverse Microscopic Anatomy of the Human Scalp. Arch Dermatol 1984; 120:450.)). Two or three hairs within this group will often merge into a common canal and protrude through a single follicular orifice (see Figure 1a). The merging of the shafts usually takes place in the infra-infundibulum of the hair follicle. Variations can be seen where the shafts share some anatomic structures with their neighbors exiting through individual but adjacent pores. The importance is not the anatomic merging of the unit but the fact that the distance between the follicular groups exceeds the width of the follicular unit itself (see Figure 1b). If these follicular units are ignored in dissection, then more skin will be transplanted than hair and significantly more skin will be moved than needed. If these groups are recognized, the implant can be “follicular” and the anatomic proximity of the hairs within each unit can be used to the surgeon’s advantage.
The advantages of using follicular implants in contrast to traditional grafts include:
- surgical wound size at the recipient site is minimized
- skin surface deformity is eliminated
- distortion due to fibrosis associated with healing is reduced
- natural scalp contour is preserved
- oxygen diffusion to implants is maximized
- interruption of blood supply is minimized
- post-op recovery time is reduced
- hair units may be placed extremely close together
- extensive numbers of implants may be moved per session
- hair may be distributed in a natural pattern
- great flexibility in recipient site design
 Figure 1a. Follicular Units (Longitudinal, Magnified: 16x)
Figure 1a. Follicular Units (Longitudinal, Magnified: 16x)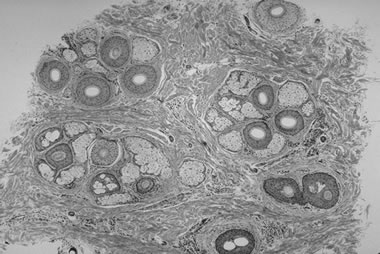 Figure 1b. Follicular Units (Horizontal, Magnified: 16x)
Figure 1b. Follicular Units (Horizontal, Magnified: 16x)NATURAL HAIR GROUPINGS
The observation of over 1,200 patients using the densitometer ((Rassman WR, Pomerantz MA: The Art and Science of Minigrafting. International Journal of Aesthetic and Restorative Surgery 1993; 1:28-29.)) reveals that in the donor area the great majority of one’s terminal hair grows in “natural hair groupings” of two, three, four, and rarely five or more hairs. These natural hair groupings are the clinical correlate of the follicular unit and have a density of approximately 10 units per 10mm2 field, supporting the view of Headington1 that the absolute number of follicular units per unit area in man appears to be relatively constant and is around one per mm2. The donor density (hair shafts per mm2), however, is quite variable and can range anywhere from 1 to 4 hairs per mm2. The number of hair shafts in each follicular unit varies for each individual and is related to the patient’s average donor density. Thus, in a patient with a high density (see Figure 2a), there would be a higher proportion of groups having 3 and 4 hairs per follicular unit, but the number of follicular units per mm2 would still be around one. In a person with low density (see Figure 2b), the predominant hair groupings might be of one and two. The presence of many hairs occurring singly is, therefore, the exception rather than the rule. To state it another way, an individual with high density does not have hair groupings closer together but has hair groupings with normal spacing between them. Each group, however, contains a greater than average number of hairs. Similarly, in a patient with low density, the spacing is not greater, only the hair groupings are smaller. As a patient ages, hairs randomly begin to miniaturize in each group so that each group will contain a combination of full terminal hairs, partially miniaturized terminal hairs, and vellus hairs (which are clinically insignificant) . Eventually, the miniaturized hairs are lost, and the natural hair groupings are reduced in number. In all adult patients, the donor area contains both terminal and miniaturized hair, indicating that this zone is not truly permanent but will thin gradually over time. It is not until the total hair density in the donor area falls below 1.5mm2 that some follicular units completely disappear, and the follicular density is seen to decrease.
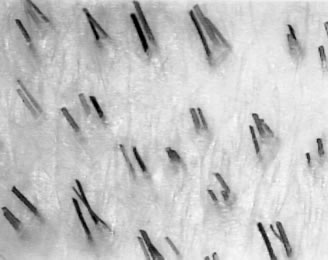 Figure 2a. Natural Hair Groupings, High Density
Figure 2a. Natural Hair Groupings, High Density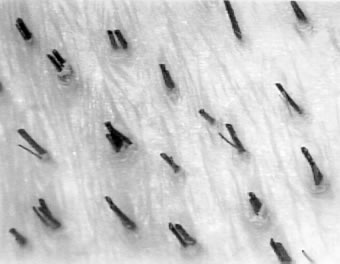 Figure 2b. Natural Hair Groupings, Low Density
Figure 2b. Natural Hair Groupings, Low DensityIn a person susceptible to androgenetic alopecia, the balding area thins in a way somewhat analogous to the donor area, i.e. miniaturized hairs gradually replace terminal hair, and the hair groupings initially decrease in size rather than in number. The major difference is that in the balding area, miniaturized hairs can populate entire hair grouping as the baldness progresses and can be so fine as to be indistinguishable from vellus hairs, whereas in the donor area there generally remain three rather distinct populations of hairs; terminal, miniaturized, and vellus. In some patients experiencing the early stages of what will eventuate in extensive balding (i.e., Norwood Class 6), where there is still some very light wispy coverage, the recipient density in these areas is surprisingly normal (i.e., close to the patient’s donor density). However, all the hairs in each follicular unit are extensively miniaturized. This underscores the fact that it is not only the absolute number of hairs but their diameter and character that contribute to clinical appearance of fullness. In the balding area, it is only after the alopecia becomes extensive and the follicular units are comprised of only one or two miniaturized hairs each, that the actual follicular units begin to disappear from the bald area.
The importance of understanding the concept of hair groupings and their age-related changes is that in order to have a natural looking hair transplant, hair placed in the recipient site should approximate that which would have been present there naturally had the individual not balded. Since the natural hair groupings in the donor area correspond to the original hair groupings in the recipient area before they were impacted by androgenic hormones, they reveal the appropriate way that this area should be restored. For example, in transplanting a 45 year old Norwood Class 6 with an average donor density of 2.2 hairs/mm2, one might try to restore the front and top of his scalp, leaving significant bitemporal recession and the crown bare. The distribution of natural hair groupings in this case might be 20% 1’s, 45% 2’s, 30% 3’s, and 5% 4’s. Therefore, attempting to place predominately 5 or 6 hair groups in this area would be destined to look unnatural. Similarly, all 1’s and 2’s in this situation would look too thin. In all situations, of course, the frontal hairline would be composed of single hair units. In the vast majority of restoration procedures, it would be appropriate to attempt to match these groupings, as they occur in nature, to produce an aesthetically balanced appearance.
WOUND HEALING
There are four related benefits to recipient site wound healing when follicular implants are used exclusively. These are minimizing the recipient site surgical wound size, eliminating skin surface deformity, decreasing the dermal fibroplasia associated with healing, and avoiding pigment alteration.
By limiting the implant to the follicular elements of the skin, the recipient site wound can be just slightly larger than the follicular unit itself so that the unit sits snugly in it. Because the follicular units are so compact, one and small two hair units have essentially the same footprint and can be placed in the same size site; and two, three, and four hair units have the same footprint and can be placed in the same size site. When the stretched slit contracts around the inserted follicular unit, the snug fit minimizes the space for a coagulum to form and reduces the distance for re-epithialization. In this situation, the fibrin “glue” will be maximally effective in securing the implant, exudate and crust formation will be reduced, and the healing time will be shortened. We instruct all patients to shampoo the day following their surgery, letting low pressure water flow over the transplanted area. This irrigation will allow the majority of patients to be free of crusting within 24 hours, requiring no dressings on the recipient area. We have found that by eliminating the crusting in one day, the surrounding erythema fades much more quickly. Within several days, most patients have faint erythema and the stubble of hair as the only clue to their hair restoration procedure.
Hair from the back and sides of the scalp grows at an angle of approximately 30 degrees. When larger grafts (which are essentially cylinders of skin and hair) are harvested, the epithelium creates an acute angle at its superior edge and an obtuse angle on the inferior edge. When the grafts are inserted into the recipient site, they must be placed at an angle that matches the angle of the original hair which vary from approximately 30 to 60 degrees. Because of this angle, mechanical forces which act on the graft immediately after placement and throughout healing, interrupt the edge-to-edge alignment of the graft with the surrounding skin causing either settling or elevation of the graft, or both. As each graft is distorted ever so slightly, the composite effect of many such grafts produces the surface irregularity (cobble stoning) of the traditional hair transplant. This surface irregularity becomes clinically more apparent as graft sizes increase and as the sites are made with punches rather than slits. This whole phenomena is simply avoided when the implants are devoid of unnecessary skin.
Slit grafting prevents cobblestoning but often produces a dimpling or puckering at the site of the emergence of the hairs by the down growth of the epidermis alongside the graft. Although follicular units are technically placed into “slits”, by reducing the perifollicular epithelium in the follicular implantation, the site required is so small (1mm) and the follicular unit so compact that this deformity does not occur.
The fibrosis that results from the healing of larger wounds causes an additional problem. Just as angulation causes surface irregularities, it also produces a distortion of the dermis that may not be readily apparent clinically. The significance of this is that grafts placed parallel do not always end up having their hair parallel under the skin surface when dermal reorganization is complete. This distortion impedes the close placement of future grafts due to the risk of damaging existing ones (even if the original angle could be exactly reproduced). This distortion of the hair shaft produced by fibrosis is easily observed each time hair is harvested and dissected from the tissue next to a previously excised donor area. Incidentally, one of the difficulties in repairing unsightly plugs by the obviously simple method of decreasing the density of the plugs with electrolysis is that the distortion of the fibrosis impedes the introduction of the electrolysis needle. The dermal changes produced by successive procedures and the difficulty in reproducing angulation are among the most compelling reasons to densely pack a given area the first time rather than to repeatedly violate a transplanted area with multiple sessions.
Another casualty of the movement of larger grafts is the melanocyte. Repigmentation after loss or disruption of the epidermis occurs by two mechanisms; migration of melanocytes from adjacent normal epidermis and migration from the follicular appendages. The presence of focal hypopigmentation at the base of larger grafts is due to the arrest of melanocyte migration into the area and attests to the fact that the grafts have produced scar tissue that has damaged both epithelial elements. The hypopigmentation at the base of the grafts often serves to accentuate any apparent plugginess by highlighting the resultant physical deformity with an additional contrast… that of color. Fortunately, hypopigmentation is less common with very small grafts and has not been observed in follicular transplantation.
CONTOUR AND VOLUMETRIC CHANGES
One of the rarely discussed but very significant cosmetic problems of grafts is the extra volume of tissue introduced into the recipient site. This extra tissue produces a fullness and elevation of the transplanted scalp and a clinically apparent ridge separating it from the surrounding bald scalp. (This condition in which the elevated area is relatively soft must be differentiated from the “hyperfibrotic changes” in the recipient area described by Stough ((Stough, DB: International Society of Hair Restoration Surgery, Third Annual Meeting 1995; Verbal Communication.)), which is a proliferative process and produces an area that is indurated.) The reason for this phenomena is that balding is not merely the absence of hair. It is an atrophic process with absence or marked diminution of entire pilosebaecous units and their associated vascularity and connective tissue support. These appendages contribute substantial volume to the normal scalp. The solution most commonly used to solve the problem of adding additional tissue to the recipient area is to cut some of the recipient area away, i.e. punch it out. Unfortunately, intact donor scalp is not the perfect match when transplanted into the bald recipient area, since it is significantly richer in each of these elements. Thus, removing skin in the recipient site is a futile attempt at compensating for the increased volume of the larger grafts, since the donor graft is much thicker than the atrophic recipient skin which it replaces. The better solution is not to transplant the intact skin in the first place, but to add only the follicular element which had been lost.
BLOOD SUPPLY AND OXYGENATION
In a “virgin scalp,” the blood supply to the recipient area is unimpeded. Each graft placed in the recipient site induces local fibrosis that interferes with normal blood flow, and every punch, large slit or ultra-pulsed laser site, has the chance to transect or seal off viable blood vessels. In subsequent procedures, the hair placed between existing grafts are implanted into scar (even though it may be microscopic) and receive the diminished flow associated with it. In follicular transplantation, the recipient site is created with a “needle like” knife that produces a minimal amount of trauma. A blood vessel that might be pierced would immediately re-seal analogous to the way a vessel heals after venipuncture. When the single hair graft is then placed into the site, the graft itself is soft and causes no additional trauma to the vessel. If it were true that a diminished blood supply would fail to support uniform graft take, then asymmetry, gaps, or areas of variable density would result from this technique and be magnified in areas of very close placement “dense packing” of grafts. However, this is not observed in spite of the fact that follicular dense packing techniques are used predominantly in the frontal hairline where any problem would be most obvious.
Since oxygen reaches the follicle by simple diffusion, oxygenation is a function of tissue mass. The larger the transplanted unit, the greater the risk that the center of the graft is impacted by the deprivation of oxygen. In contrast, the barrier to oxygen transport is at a physiologic minimum with the follicular implant. In this respect, the follicular implant should have enhanced survival and the phenomena of “doughnuting” seen with larger grafts can be avoided. In addition, since the follicular unit sits snugly in the recipient site, there is a minimum amount of coagulum impeding diffusion from the dermal blood supply to the edge of the graft.
TRANSPLANTATION IN EXTENSIVE QUANTITIES
Once the question of implant size is resolved, the corollary issue is the necessity of transplanting extensive quantities of these implants in a single or very limited number of sessions, given its medical feasibility. A simplistic answer is that when graft size decreases, the number of grafts must increase to yield the same amount of hair, which of course is true. However, there are a host of more compelling reasons to perform transplants in large sessions.
Putting aside anatomic, physiologic and technical issues for the moment, it is important to emphasize the social and practical reasons to strive toward large sessions. The majority of patients who seek hair restoration surgery feel that their balding interferes with their life either socially, professionally, or both.
Until the hair restoration surgery reaches a point where there is acceptable cosmetic improvement, the patient will be focusing more on his hair loss than he did before. Multiple, small procedures spaced out over an extended period of time keeps the patient focused on the very problem he wanted to correct. During this period, his self-consciousness worsens and disappointment begins when he realizes that limited procedures fall short of his expectations. Even in the emotionally secure individual, the disruptions in daily life from the scheduling of multiple surgeries, the resultant limitations in activity, and the concern about their discovery can cause undue stress. In addition, post-operative numbness and paresthesias in the posterior scalp are constant reminders of the operation.
Multiple, partial procedures produce short-term cosmetic problems. The planning of rows of grafts that must be filled in at a later time to look normal or to be camouflaged by subsequent rows of micrografts is certainly not appreciated by the patient seeking cosmetic improvement. Flaps, multiple-staged scalp reductions, and those requiring tissue expansion certainly fit into this category as well. often the cosmetic appearance of the work is only acceptable because the patient’s own hair camouflages it. Patients undergoing multiple procedures in such a cosmetically visible area as the scalp can be so discouraged that they give up on the process entirely. In fact, many do stop until their baldness progresses and their own hair becomes unsuccessful in camouflaging the surgery. They then re-enter the population of partially treated patients shifting from doctor to doctor seeking someone who will finish the procedure. There is an important distinction between a person in the early stages of balding, undergoing a hair transplant, who has been well-informed that future procedures will be required as he balds further and a patient who begins hair restoration unaware that during an extended surgical process his appearance may be totally unacceptable to him and that he may never reach his goal.
With respect to medical feasibility, follicular transplantation is qualitatively, as well as quantitatively, different from traditional grafting; therefore, the mere extrapolation from the older techniques will not allow one to predict the outcome of the newer procedure. The physiologic limitations to transplanting large numbers of traditional grafts, such as the impediment of blood flow and interference with oxygenation as discussed above, clearly do not apply when dealing with the movement of small follicular implants. Experience has shown that up to 3600 or more follicular units may be moved safely in one session with the main limitation being the donor supply rather than the physiology of the recipient area.
The surgical issues favoring large sessions are significant. Virgin scalp has normal collagen and normal blood flow. If possible, one should transplant the total number of required grafts in the first session to take advantage of this environment. Successive implantation into a previously treated area is always hindered by the angle of the existing grafts, distortion due to fibrosis, and altered vascularity. Although follicular implantation can minimize these factors, it certainly cannot reduce them to zero. In addition, the spacing, orientation, and distribution of the implants can be planned in an unrestricted fashion without these parameters being controlled by their relationship to existing grafts.
In virgin scalp, the dermis retains its normal distensibility, therefore, implants can be placed closer together with less tendency for “popping” of adjacent units. During the post-op period, the implants will be less likely to elevate or settle as healthy collagen and elastic fibers grasp the transplanted units firmly and add to the glue-like properties of the coagulum in securing the implants.
Hair transplantation often produces varying degrees of telogen effluvium in the recipient area. This hair loss can be substantial in the young patient who is rapidly balding and whose recipient area is characterized by a high degree of miniaturization. often this lost hair does not return. Unless a significant amount of hair is transplanted in these individuals, the gain from the surgery may not even be adequate to compensate for the loss due to the telogen effluvium.
Large sessions also offer an advantage over multiple small sessions in the donor area. Each time grafts are harvested from the donor area, there is loss of potential donor hair due to destruction of hair adjacent to the wound edges from the fibrosis associated with primary intention closures. In addition, the hair follicles adjacent to the healed suture line are often distorted and more difficult to harvest on subsequent procedures causing an increased number of hairs to be transected . Minimizing the number of times the donor area is accessed will obviously minimize the distortion and wastage due to the closure.
THE DONOR BANK
There are two processes that occur simultaneously in the balding individual. One is androgenetic alopecia, i.e. the patterned hair loss programmed to affect only certain hair follicles in susceptible individuals, and hair loss due to aging itself, which to some degree affects all hair in everyone. The donor region in the back of the scalp where hair is traditionally harvested from has been optimistically called the “permanent zone”; however, this zone is far from permanent. It may be spared from the process of genetic balding, but it is surely affected by the aging process itself. It seems that on the average the donor site thins at least 30% over one’s lifetime due to simple aging. In some men with extensive balding, the permanent hair seems to be affected by the genetic process as well, and when these two processes occur together, the decrease in donor density can be marked with counts occasionally falling below one hair/mm2. This process is probably analogous to the extensive diffuse thinning seen occasionally in women. The continued loss of hair in the permanent zone over time must, of course, be accounted for in the planning of the hair transplant and in giving a realistic prediction to the patient of the long-term stability of the transplanted hair.
Two major factors determine the amount of hair that can be safely removed from the donor area. The first is donor density, and the second is scalp laxity. The importance of accurately assessing donor density cannot be over emphasized. At the initial consultation, density determinations are made from a representative area in the permanent zone where the donor strip might be harvested. If there is significant clinical variability in the donor density or scarring due to prior surgery, then multiple measurements are taken. These numbers are used in the initial planning of the procedure. At the time of surgery, the density is measured again, calculations are taken to determine the length and width of the donor strip, and the area is then prepped and shaved. The shaved donor site is then inspected for irregularities of density due to natural variability and those resulting from scarring due to past procedures. Multiple determinations are made again and averaged to accurately assess the density. Our experience has shown that the gross visual impression of density is often at variance from the true density by a factor of up to 35% and is far too imprecise to be useful in surgical planning.
Scalp laxity is a more subjective measurement, but with experience can be estimated with a reasonably high degree of accuracy. Judging scalp mobility by simply moving the scalp up and down with the hand or tenting of the skin between the fingers are the two obvious means of assessing laxity. Also useful is noting the thickness of the scalp (an abundance of subcutaneous fat makes for a mobile scalp) and observing the configuration (contour) of the cranial bones. Prominent mastoid processes and occipital notches decrease the ability to easily close a horizontal incision. We use a Rassman knife that when fully loaded with 8 blades produces a strip 21mm in width. By removing blades, one can harvest strips of 18mm, 15mm, 12mm, 9mm and so on. Generally, the widest strip that can be harvested without producing undue tension during closure should be used. If a strip is too narrow, then its length must be increased to yield the same amount of hair and a longer incision produces more donor site scarring and distortion. If a strip is too wide, then tension on the wound edge may result in dehiscence, infection, excessive post-operative discomfort, prolonged wound healing or a hypertrophic or spread scar. In general, the greatest degree of tension occurs over the mastoid processes, and great care should be taken when estimating scalp mobility in this location. If it is anticipated that this area will be a limiting factor in the harvest, then it is best to use a more conservative width and excise a longer strip. In patients having a very prominent occipital protuberance, the greatest tension may be at the midline. In this situation one may either remove a blade to narrow the width as one extends medially or to harvest an additional strip on one or both sides freehand. On occasion, when a patient with a prominent ridge has had multiple previous surgeries, the strip is harvested in two separate pieces neither extending to the midline.
The plane of dissection should be just below the hair follicles in the superficial fat to avoid damaging the larger nerves and blood vessels which lie deep in the subcutaneous layer, just above the galea apounurotica. If possible, the galea should not be violated as this fibrous band serves as the structural support of the wound closure and prevents its spread. Suturing a transected galea will never approach the strength of the membrane left intact. In addition, dissection in the subcutaneous layer avoids the necessity of a layered closure and its associated foreign body reaction. In very large sessions where up to 50 square centimeters of scalp may be removed and the incision length can be 30 cm, the importance of superficial dissection and leaving the galea intact cannot be over emphasized. In addition, we never undermine. In the rare instance where the wound edges cannot be approximated, it is better left to heal by secondary intention rather than to risk damaging hair follicles, blood vessels or nerves. Any cosmetically unacceptable scar can easily be removed in the future after the scalp tension has decreased. We also do not electrodessicate. Bleeding generally occurs at the wound edges and is controlled with a running cutaneous suture. On rare occasion, a larger vessel is ligated using 4-0 Vicryl, if it would not be incorporated easily in the closure.
We use a single running suture of 2-0 polypropylene. The sutures are generally left in place for two weeks. However, if there is significant tension during the closure then these sutures may be left in place for three or more weeks as polypropylene produces little tissue reactivity. The entire length of the suture line is kept covered continually with a topical antibiotic in an ointment base (Bacitracin). At the time of suture removal, the sutures should protrude slightly above the scalp surface which indicates that edema and inflammation have significantly subsided. This is in sharp contrast to sutures left in glaborous skin, which become progressively more embedded the longer they are left in place. In patients without penicillin sensitivity, we pre-medicate with Dicloxacillin 1gm PO, 1 hour prior to surgery, and then a second dose of 500mg PO 6 hours later if there was excessive bleeding, or wound tension. ((Haas AF, Grekin RC: Antibiotic Prophylaxis in Dermatologic Surgery. JAAD 1995; 32:155-164.))
In determining the position of the donor incision, it is best to assume that the patient may become a Norwood Class 7; therefore, the hair transplant surgeon should place the upper blade of the rake at least 1cm below the lowest point of possible hair loss. This will allow for coverage of the scar in the worst case scenario. As the incision extends laterally, it should be at least 1 cm superior to the top of the ear. It is important to stay very superficial in this area, especially as one extends the incision towards the temples, as the parietal branch of the superficial temporal artery and vein as well as branches of the auriculotemporal nerve lie very close to the undersurface of the dermis in this location. ((Salasche SJ, Bernstein G, Senkarik M. Surgical Anatomy of the Skin. Norwalk, Connecticut: Appleton and Lange, 1988 pp 176-177.)) The excision should not extend anteriorly to a position closer than 3 cm from the hairline. Some patients may have extensive bitemporal recession, and this should be anticipated by carefully assessing the extent of the patient’s current recession, the degree of miniaturization at the free edge, and the family history.
Traditional surgical techniques have often left a “step-ladder” pattern of scarring in the donor area. When there is a preexisting horizontal linear scar (or scars), the scar may be totally avoided, totally incorporated into the new strip, or incorporated into one edge of the new incision. If the scar is in a position where it is already placed too high and may possibly be exposed with further balding, it is best avoided. If the scar had been placed too low, it is also best avoided to reduce the chance of hypertrophic scarring. Also if the donor area is relatively tight from prior surgery and if the scar is not visible, it may be left in place, as removing it will only increase wound tension. Avoiding the scar will maximize the yield of hair for that particular procedure. One may totally incorporate the scar if it is clinically visible and if there is enough laxity to remove it and still obtain the desired amount of hair. It is critically important to ascertain why the patient scarred in the first place. If the scar was a result of poor surgical technique and the problem can be identified and corrected, then excising it may be appropriate. If the scar (either stretched or hypertrophic) was due to the intrinsic healing properties of the individual (as seen in Ehlers-Danlos syndrome), then the scar is best avoided, because removing it will further increase wound tension, and the problem will most likely reoccur. It is important to assess the impact of the scarring on the average donor density as small amounts of scarring can significantly decrease hair yield due to distortion of follicles in the surrounding area. In the majority of instances, we opt for the third choice i.e., using the previous scar as the upper or lower boarder of the new excision. We will remove all but approximately 1.5 mm of the width of the scar to allow the suturing to be limited to the scarred area and not to extend into viable hair bearing scalp. In this way the amount of distortion and possible damage to existing hair is limited to only one free edge.
Strip Length
Accurately estimating the size of the donor strip and the amount of hair that it will contain is more difficult in follicular transplantation but also more important because of the large tissue requirements. We find that precise measurements are essential in this regard. As in the assessment of density, a clinical “feeling” about the size of the strip needed is far too imprecise to be relied upon to guide the surgery. To calculate the length of the donor strip we use the following equation (A), or its derivative (B):
Example:
1. Decide upon the total number of follicular units needed for the transplant (see section on Design of The Recipient Site).
2. Using the densitometer, measure the patient’s donor density (in mm2 ) and observe the patient’s natural hair groupings. (If a patient has had prior surgical procedures and the harvesting will be in an area of scarring, estimate the proportion of that area that has been replaced by scar (DS). Remember that the effects of the scarring in reducing donor density will extend slightly into the adjacent hair bearing area due to the follicular distortion that the scar produces. In addition, the size of the follicular units are often decreased in areas of scarring so that it is not uncommon to see a preponderance of 1’s in these areas.)
3. Calculate the number of hairs needed based upon the desired total number of follicular units, the proportion of 1, 2, 3, and 4 hair follicular units, and the total number of hairs they will yield.
For Example: If you plan to transplant 2,500 FU’s and the patient has a donor density of 2.2 with 15% of the area affected by prior open donor techniques and has 20% 1’s, 45% 2’s, 30% 3’s, and 5% 4’s, you may want the cutters to produce 500 1’s for the frontal hairline, and 1100 2’s, 800 3’s, and 100 4’s behind the frontal hairline and on the top of the scalp.
The total number of hairs needed in this patient are:
| # of Units | x Unit Size | =# of Hairs |
| 500 | x 1 | = 500 hairs |
| 1100 | x 2 | = 2200 hairs |
| 800 | x 3 | = 2400 hairs |
| 100 | x 4 | = 400 hairs |
| 2500 | 5500 | |
4. Estimate the Correction Factor (CF). The correction factor is unique to each surgical team and is an estimation of the fraction of grafts lost from harvesting the strip, the loss from dissection of the individual units, and errors due to visual limitations in identifying the hair. (In this example the CF = O.3.)
5. Estimate scalp laxity and decide on the number of blades to be used.
6. For harvesting we use a Rassman Handle, 8 Blade 2.7mm, loaded w/2-8 Personna Plus # 10 Blades, which produces strips 3mm wide. The total width of the strips = (# blades – 1) x 0.3 cm or (# strips) x 0.3 cm (In this example 7 blades are used).
7. Multiply the denominator by 100 to convert mm2 to cm2.
In patients that have NO prior scarring due to surgery
Finally, when there is no donor scarring, and the donor density is over 1.5/mm2, the follicular units are intact and the normal follicular density is equal to 1/mm2 (see section on Natural Hair Groupings). The equation then further reduces to:

In the above equation, the calculation of strip length becomes independent of donor density. The explanation of this apparent paradox is simple. If, in the above example, one wanted to transplant 2,500 follicular units, and the harvesting and dissection were flawless, one would need exactly 2,500 mm2 or 25cm2 of donor tissue (since the follicular density in normal situations is constant at 1/mm2). In patients with a higher donor density, one would still transplant 2500 follicular units, but each unit would now contain a higher number of hairs, giving greater recipient density. The converse would be true for patients with low donor density. The question that logically follows is “Why bother to take densitometry readings and calculate donor density in the first place?” The reason is that densitometry measurements reveal the composition of the follicular unit and the donor density is actually a measurement of the average size of these units. Thus, a patient who has a donor density of 2.2/mm2 actually has follicular units containing an average of 2.2 hairs each. It is the composition of the follicular unit that ultimately guides the design and planning of the hair restoration.
Density and Donor Supply
An accurate assessment of the total moveable donor reservoir of hair is critical for long-term planing. In our experience, the average donor density for all patients (both bald and non -bald) seeking a consultation for hair restoration surgery have an average donor density of 2 hairs/mm2. In general, for individuals with straight hair of average diameter, the donor density must be at least 1 hair/mm2 in order to adequately cover the donor area and not have it appear too thin. A density of 1 hair/mm2 is also the minimal density needed to hide an average donor scar. If a patient has wavy or thick hair the minimum density may be slightly less and in patients with very fine, straight hair the minimum density will be more.
The limitations placed upon the amount of harvestable donor hair due to these minimal density requirements needed to cover the donor area, create a relationship between donor density and donor reservoir that is not one to one. A unit change in donor density away from the norm will produce a two-fold change in the availability of transplantable hair. For example, compared to the average person (with a donor density of 2.0), a balding individual with a donor density of 2.7 (which is a 35% increase) will have 70% more hair available to transplant. Conversely, a person with a donor density of 1.3 will have 70% less transplantable hair, and may not be a candidate for surgery regardless of his Norwood classification. If he were to bald extensively, almost any type of surgical hair restoration would leave him desperately short of hair and short on coverage in the donor area. Unless the hair restoration surgeon is aware of this relationship, miscalculations will be made when relying on absolute donor density in assessing total donor supply.
The relationship between donor density and total available donor hair ((Rassman WR, Carson S: Micrografting in Extensive Quantities, The Ideal Hair Restoration Procedure. Dermatologic Surgery 1995; 21:306-311)) in an individual with straight hair of average diameter is illustrated below (Table 1).
The importance of using the densitometer in assessing donor supply cannot be overemphasized. With multiple procedures, each harvest decreases the remaining donor density, and this measurement, together with the decrease in scalp laxity, will give a good indication of what can be achieved in the subsequent surgery. Women with non-patterned diffuse alopecia often have donor densities in the range of 1.0 to 1.5, and for similar reasons are also not good candidates for transplantation.
PREPARATION, HANDLING, AND PROJECTION of THE FOLLICULAR IMPLANTS
The basic concept in dissection is to identify the patient’s natural hair groupings and to isolate individual follicular units. A delicate balance must be reached between the goal of having the implant purely follicular and leaving enough peri-adventitial stroma to ensure that the implant is not damaged and hair is not wasted. This balance is achieved through the extensive experience of a highly motivated staff that are trained specifically for this task. Because the implants are so small, they are more sensitive to desiccation and temperature change. Therefore, handling and quality control at every level of the procedure are crucial to obtaining good results.
The initial harvest scores the strip just below the level of the hair follicles into 0.3 cm wide longitudinal sections with each attached to the other by the loose connective tissue of the subcutaneous layer. The sections are cut into pieces 1 cm in length. Each piece is then further subdivided, and the follicular units are identified, under magnification, and dissected free of surrounding skin. We prefer a #10 Personna blade and cut on tongue depressors that have been soaked in sterile water (not saline) until they are ready to be used. Immediately before use the excess water is removed with a piece of gauze. The purpose of soaking is to help maintain the moisture of the implants and to prevent the tongue depressors from absorbing water from the saline soaked implants, thereby increasing the relative concentration of the saline.
Dissection of the follicular units is the most labor intensive and critical part of the follicular implantation process. We use up to 12 highly trained cutters to produce the implants for a single large case. Proper planning of the recipient area is absolutely dependent upon accurate information regarding the yield of the donor harvest. The dilemma in planning is that waiting until all the units are dissected before implanting extends the length of the surgery beyond medical feasibility and starting before the surgeon has information about the total number of 1, 2 and 3 hair units, limits the ability to make precise decisions regarding size, density and distribution of the recipient sites. Although it would seem that information gleaned from pre-operative densitometry measurements together with the patient’s hair characteristics and the calculations described above would be adequate for the creation of the recipient sites, in actuality, once the dissection begins, new crucial information is obtained. For example, patients with gray-white hair can have either dark or light roots. In the latter case, due to decreased visibility, the cutters must leave more stroma around the units, increasing the implant size. As a result, a two-hair implant might require the same size site as a three-hair unit. On the other hand, in patients with fine hair, two hair units may be placed in a site made to accommodate single hairs. In patients with kinky hair, the hair shaft is often so curved below the level of the skin that close dissection of the units is impossible… but sometimes it is not, and the kinky hair behaves during dissection as if it were straight. In all cases, the smallest possible site is used for the respective implant in order to minimize injury to the recipient site and to allow for the very close placement of the follicular units.
In order to take into account these variables, the staff is instructed to take random pieces from the cut strip, and representative units are matched with sample sites. Placing of sites is then limited to the frontal hairline until the first projection of the implants is made (Table 2). Accurate projections of the total number of units that will be obtained from the donor harvest are critical for the correct placement of the sites with respect to size, density and distribution, allowing the creation of sites to proceed while the cutting is still in progress.
Table 2. Follicular Unit Projection Worksheet. A sample of the projection worksheet used by our staff. In the example that follows, a strip removed with an eight bladed scalpel measuring 2.1cm x 24.2cm was subdivided into 142 pieces prior to dissection.
PROJECTION WORKSHEET
Patient’s Name ___________________ Date _________ Suite #______
Case Organizer _________________
Count #: _____
CUT: ____ corners _____ pieces
TOTAL: _____ corners ______ pieces
Cutters: 1’s 2’s 3’s 4’s TFU’s
1 ____ ____ ____ ____
2 ____ ____ ____ ____
3 ____ ____ ____ ____
4 ____ ____ ____ ____
5 ____ ____ ____ ____
6 ____ ____ ____ ____
7 ____ ____ ____ ____
8 ____ ____ ____ ____
9 ____ ____ ____ ____
10 ____ ____ ____ ____
11 ____ ____ ____ ____
12 ____ ____ ____ ____
Sum of cut pieces: ____ ____ ____ ____ = ______
Number of cut pieces: ____
Average units per piece: ____ ____ ____ ____ = ______
Average x total pieces ____ ____ ____ ____ = ______
Corners (2) ____ ____ ____ ____ = ______
Total Projected ____ ____ ____ ____ = ______
Instructions:
To project the number of follicular units (FU’s):
1. Cut both corners and then begin to cut pieces.
2. Take an estimate after both corners and approximately 20% of the pieces have been cut and subsequent counts as
required by the size of the case.
3. Count 1, 2, 3, 4 and Total FU’s of corners and keep these numbers separate.
4. Count 1, 2, 3, 4 and Total FU’s, of the cut pieces, divide by the number of pieces cut to find the average number
of units per piece. Then multiply the average of each piece by the total number of pieces.
3. Add 1, 2, 3, 4 and Total FU’s of corners + projected 1, 2, 3, 4 and total FU’s of pieces = PROJECTION.
Both the cut pieces and individual implants are held in 0.9% Saline chilled to 59of. They are never out of chilled solution longer than 3-5 minutes. The placers rest a small amount of follicular units on back of the opposite hand used to hold the forceps. The placers wear powder-free gloves and place gauze under the glove beneath the area where the moistened implants will lie to prevent heat transfer from the hand into the implants. Implants are inserted with curved jewelers forceps. At the beginning of the placing, each assistant will determine his placing speed, which depends upon their skill and the patient’s specific hair and scalp characteristics. Once they have determined their speed for the specific case, it is easy for them to determine the amount of grafts that can be safely handled at any one time.
Hydrogen peroxide is very effective in removing residual blood from the scalp and acting as a mild hemostatic agent through a variety of possible mechanisms, ((Larson PO: Topical Hemostatic Agents for Dermatologic Surgery. J Dermatolgic Surg. Oncol. 14:6 1988.)) and although it seems to produce little significant toxicity in normal usage, we exercise great caution during follicular transplantation and avoid its direct use on viable tissue. Fortunately, hydrogen peroxide is rapidly broken down to oxygen and water. In order to minimize its contact with the implants or with open wounds, we never spray or apply peroxide directly to the scalp. We use a 3% hydrogen peroxide solution diluted to 1 part hydrogen peroxide to 4 parts water, making an effective concentration of hydrogen peroxide of 0.6%. Any bleeding in the recipient area is stopped by applying direct pressure with dry gauze, not with peroxide. After the bleeding has subsided, 3×3 gauze is sprayed with the diluted peroxide and then applied to the skin to remove residual blood.
DESIGN OF THE RECIPIENT AREA
In Follicular Implantation, we use five major elements to guide the creation of the recipient sites:
1) produce a natural pattern
2) frame the face and spare the crown
3) eliminate contrast
4) have the hair emerge at natural angles, and
5) have a natural distribution of follicular units.
Although an in-depth discussion on design is beyond the scope of this article, we would like to briefly explain the importance of these elements.
Natural Pattern
To a large extent, the correct template for hairline placement, hair distribution, and density has already been supplied by nature. The closer one follows the pattern set by nature, the more natural the hair restoration will appear. A hair transplant no matter how dense or how perfectly executed will look artificial unless it produces a look that others can recognize as one they had seen before. Just as the follicular implant attempts to mimic the way hair grows in nature on a microscopic level, the overall design of the follicular implantation should strive to mimic nature on a gross level.
The power of “The Isolated Frontal Forelock” recently described by Marritt and Dzubow ((Marritt E, Dzubow L: The Isolated Frontal Forelock. Dermatologic Surgery 1995;21523-538.)) lies in the fact that they identified a pattern seen in nature that was reproducible within the limits of the patient’s donor supply. However, the use of larger grafts for the dense posterior component limits the amount of available donor hair, and creates a natural look only when disguised by the anterior component. The main limitation of flaps and scalp reductions (even in the best of circumstances where there are no complications) are that although they achieve high density, there is no natural counterpart to the distribution they produce. Flaps bring the patient’s donor density to the frontal hairline, with a sharp demarcation anteriorly and posteriorly, a pattern never seen in nature. This area of high density must then be supported by a similar density around it to look natural and, of course, if the patient had enough hair to accomplish this, he wouldn’t have needed hair restoration in the first place. The scalp reduction, although appealing on a superficial level (“remove the bald area so there will be less area to transplant”), violates the same rules of nature as does the flap. A scar is placed in an area that should have light coverage (if any), the direction of hair is changed, the pattern of future balding of that crown will be altered, and donor density is decreased. In effect, scalp reductions are a “crown transplant” and thereby reduce the hair available for the cosmetically more important front.
We feel that the optimal way to plan a hair transplant procedure would be to first assess the patient’s present pattern of loss and to anticipate his possible future pattern (considering his present age and familial hair loss patterns) using the worst case scenario as a reference point. Next, determine a person’s total donor reservoir of hair (taking into account absolute donor density, degree of miniaturization, hair groupings and scalp mobility). Then, carefully analyze his specific hair characteristics which affect the appearance of fullness and naturalness (such as wave, hair shaft diameter and skin/hair color contrast). With this information in hand , one can realistically plan how far back in time one can go along his hair loss continuum, given the patient’s particular resources.
For example, a 55 year old Norwood Class 4 with a donor density of 2.3 and 20% miniaturization in the donor area and wavy hair, may be safely restored to a Class 3 using 1700 follicular units (Table 3). On the other hand, a 23 year old Class 5 patient with a donor density of 1.9 and 35% miniaturization in the donor site, with fine, straight hair should be restored to a Class 3 Vertex, rather than a regular Class 3. using 1500 follicular units. In this situation, we would use 1500 follicular units and leave the crown untreated. If he were to bald extensively, he might end up years later with an isolated tuft of hair in the crown, without enough donor reserves to complete the hair transplant.
Frame The Face and Spare The Crown
The patient judges the success of his hair restoration by its ability to enhance his appearance, which is in large part based upon the ability of keeping his facial features in proportion. In this regard, the second important element in proper planning is to make every effort to “frame the face”. Transplants which add density to a hairline placed too high (in the hope of conserving donor hair) only accentuate the patient’s baldness by elongating a bald forehead. It frames the forehead rather than the face. We generally place the frontal hairline one fingerbreadth (2cm) above the uppermost brow wrinkle (mature hairline). It is important to differentiate this from the patient’s original hairline which sits directly above the brow wrinkles, lacks bitemporal recession, and should not be used as a landmark for planning the hair transplant. When the donor supply is limited, it is much better to compromise towards the crown than to compromise the critically important position of the frontal hairline.
The decision to transplant the crown is an important one, because compared to other areas of balding, it is the least visible but occupies the greatest area. The progressively balding crown can produce huge demands upon the donor supply, and because this area is also the least stable, hair must always be reserved for this eventuality. Furthermore, the crown expands centrifugally, rather than in the predominantly anterior-posterior direction of the front and top, with the center of the crown always having the least amount of hair and being surrounded by areas of increasing densities. Because of this, any hair placed in the center of a balding crown can result in an island of hair surrounded by a moat of bald skin. To correct this, hair of increasing density must be added around it to be aesthetically balanced, consuming vast amounts of hair that could be better saved for the front. Because of these issues, we generally reserve treatment of the crown for older patients with above-average donor density and stable hair loss of Class 3 Vertex, Class 4, and Class 5, or patients of Norwood Class 6 with high donor density and good scalp mobility (Table 3). If extensive balding is a possibility, it is always best to treat the crown as an extension of the top, rather than as an isolated region to ensure that you will not be short of hair if the intervening region were to bald.
Eliminate Contrast
The next element in planning the follicular transplantation is the elimination of contrast. We have already gone to great lengths to illustrate how eliminating contrast on the “micro” level is important, i.e. eliminating the contrast between the individual graft and the surrounding skin. It is equally important to eliminate contrast on the “macro” level, i.e. between one part of the scalp and the other. One of the most striking features about the balding process is that practically all of the Norwood Class A patients look aesthetically worse than their regular Norwood counterparts. In fact, most Norwood Class A patients look worse than patients in the next higher Norwood Class, in spite of the fact that those patients have more hair. Thus, a Norwood Class 4A often looks worse than a Class 5, and a Norwood Class 5A often worse than a Class 6. Clinically, we find that the Class A patients are often the most distraught over their hair loss and benefit most from the hair transplant procedure.
The reason for this is simple. In the Class A patient, there is the greatest contrast between the hair bearing area and the totally bald scalp. Curly or wavy hair increases the clinical appearance of density. In the regular Norwood classes, a curly or wavy haired patient will look less bald, because any slight coverage on top will be magnified by the character of the hair. In contradistinction, curly or wavy hair will make the Class A patient look more bald, because in this patient it will accentuate the contrast.
The same reasoning helps to explain why an older patient looks better as a Class 6 than a younger patient. The younger patient has had patterned androgenetic effects causing hair loss in the bald area. His donor density is essentially unchanged. The older patient, however, has had hair loss due to both patterned androgenetic balding as well as loss due to the aging process itself, the latter affecting the “permanent zone”. In addition, the older patient has a higher degree of miniaturization in the donor area, which further reduces the contrast.
Furthermore, the younger patient with higher donor density will look more bald than his Norwood counterpart with lower density. In patients of all ages where the bald area is too extensive to be covered by adjacent hair, the patient’s cosmetic appearance is generally enhanced by keeping the hair short, which is just another means of decreasing the contrast between the two areas. Fortunately, the higher the density of the permanent zone, the worse the bald areas look in comparison, but the more hair there is available to transplant. In a sense, hair transplants do not add hair, they decrease contrast by moving hair around.
Angulation
The single most useful clue to proper angulation is to observe the patient’s existing hair. Even in very bald areas, a few vestigial hairs will often indicate the original orientation of the terminal hair. When this information is not available, the safest direction to follow, aside from the crown, is generally forward. The majority of hair anterior to the crown points forward with the angle becoming more acute anteriorly. The direction of the frontal hairline is also forward, rather than radial, and only deviates significantly from this as one approaches the temples. Horizontal placement of the frontal hair is usually appropriate, regardless of the slope of the forehead.
Follicular implantation provides almost unlimited freedom in choosing the angle at which the future hair will emerge from the scalp. This is because the mechanical forces facing the larger grafts placed at acute angles do not affect the follicular implant. The delicate swirl of the crown, the abrupt directional changes of the cowlick, and the sharp angulation of the temples, can all be re-created with follicular implants. The challenge is not merely creating these angles, but observing the myriad of patterns seen in nature so that this variety can be duplicated for our patients.
Distribution
In almost all cases of balding, there is a rationing of donor hair due to the necessity of covering an ever expanding recipient area with a much smaller, but finite, donor supply (Table 3). We try to evenly space the individual units in a random rather than grid-like pattern and always try to increase the density in the areas of cosmetic importance. In doing so, we remember the adage “To cover a baseball field with grass, use seed rather than sod….., and if you only have a limited amount, use it in the infield.”
Table 3. Follicular Units in Hair Transplant. The total number of follicular units generally transplanted in the first session for specific Norwood classifications are listed. In general, the higher the donor density, the greater the number of hairs each follicular unit will contain. With low donor density, little scalp laxity or poor hair characteristics, these targets may not be achievable.
* See text for indications.
** We generally do not recommend hair restoration surgery for Class 3 patients unless the hair loss is cosmetically very bothersome, the pattern seems to be stable (i.e., low degrees of donor and recipient site miniaturization), and higher than normal donor density. Often these patients have special circumstances, such as career demands, which require transplantation at an early stage. Informed consent should be obtained regarding the commitment to further surgery if the hair loss progresses.
THE FUTURE
We began this article by stating that “Follicular Transplantation is the logical end point of over 30 years of evolution in hair restoration surgery”. Although working at the follicular level may be an end point with regard to size, it by no means implies that our work is complete. We feel that a few exciting new areas deserve mention.
The first is the use of ultra-pulsed CO2 laser systems. The major advantage that lasers are purported to have over traditional slit and punch grafting is that they can create a slit while at the same time removing recipient tissue, like a punch. In follicular transplantation, the implant is already trimmed of excess tissue, therefore, this is of little value. In addition, the laser slit is far too large to grasp the tiny follicular implant. Most importantly, the laser seals the microscopic vasculature while removing tissue. It is the relative preservation of this critical recipient blood flow that makes follicular implantation such an appealing process and allows for the survival of extensive numbers of implants. As laser technology improves and the issues of spacing and thermal injury have been adequately addressed, the advantage of rapidly producing large numbers of uniform slits may make the laser a more valuable tool.
The second is video-imaging. The video-imager ((Transplant Videografting System of the Professional Hair Institute; displayed at the International Society of Hair Restoration Surgery, Third Annual Meeting 1995.)) is actually a sophisticated densitometer, and because of its very high resolution (up to 200X) and its photographic capabilities, it is a means by which implants can be assessed for physical damage, hair counts can be more accurate, and the question of graft survival and yield can be addressed in a scientific way.
Finally, the area of automation should have the greatest impact on hair restoration surgery in the near future. Follicular transplantation is a labor-intensive procedure making huge physical demands on the hair transplant surgeon and staff. Instrumentation currently being developed will streamline the entire process from the harvesting of the donor strip, to the insertion of the implants. With certainty, these future developments will increase the speed and lessen the manpower required in the hair transplant process. If they can also increase the quality of our results, we will have a better, more affordable treatment to offer our patients.
GLOSSARY OF TERMS
Follicular Unit – the unit of tissue moved in the follicular transplantation process, consisting of a hair follicle, associated hair shafts and peri-folliculum.
Follicular Implant – the follicular unit that has been placed in a recipient site created by a puncture wound just large enough to accommodate it.
Follicular Transplantation – a method of hair restoration surgery by which follicular implants are harvested, prepared, and placed in accordance with long-term strategic planning of design to maximize
the cosmetic benefit to the patient throughout his lifetime.
Grafts – skin and hair moved in the hair transplantation process in which the transplanted tissue contains approximately the same ratio of follicles to skin present in the donor area.
Mature Hairline – the adult hairline that has not yet shown the effects of genetic balding. At the midline of the forehead, it generally begins 2 cm above the uppermost brow wrinkle.
Modified NoKor – a standard 18 gauge NoKor needle that has be modified so that the blade is 1 mm in
diameter. Its specific use is for the creation of single hair recipient sites in patients with hair of average diameter and for one and two hair units in patients with fine hair.
Miniaturization – the progressive diminution of hair shaft size often associated with the loss of pigment due to genetically determined effects of androgenic hormones on the hair follicle.
Natural Hair Groupings – the number of hairs naturally growing together due to the anatomic fusion or association of individual hair shafts. These hairs may share anatomic structures and emerge from a single or adjacent follicular orifices.
Original Hairline – the teenage or adolescent hairline which is generally flat, i.e., does not show bitemporal recession.
REFERENCES
- Headington JT: Transverse Microscopic Anatomy of the Human Scalp. Arch Dermatol 1984; 120:450.
- Rassman WR, Pomerantz MA: The Art and Science of Minigrafting. International Journal of Aesthetic and Restorative Surgery 1993; 1:28-29.
- Stough, DB: International Society of Hair Restoration Surgery, Third Annual Meeting 1995; Verbal Communication.
- Haas AF, Grekin RC: Antibiotic Prophylaxis in Dermatologic Surgery. JAAD 1995; 32:155-164.
- Salasche SJ, Bernstein G, Senkarik M. Surgical Anatomy of the Skin. Norwalk, Connecticut: Appleton and Lange, 1988 pp 176-177.
- Rassman WR, Carson S: Micrografting in Extensive Quantities, The Ideal Hair Restoration Procedure. Dermatologic Surgery 1995; 21:306-311
- Larson PO: Topical Hemostatic Agents for Dermatologic Surgery. J Dermatolgic Surg. Oncol. 14:6 1988.
- Marritt E, Dzubow L: The Isolated Frontal Forelock. Dermatologic Surgery 1995;21523-538.
- Transplant Videografting System of the Professional Hair Institute; displayed at the International Society of Hair Restoration Surgery, Third Annual Meeting 1995.



