
AESTHETIC ISSUES
The Frontal Hairline and Other Transition zones
Determining the position of the hairline and the importance of considering the vertex transition point in the long-term plan have been discussed in the section “Planning the Restoration.” The transplanted hairline must be restored to a position appropriate for a mature adult since, in contrast to one’s original hairline, it will not change its position or shape over time.
In a mature adult, the mid-portion of the frontal hairline is approximately one finger-breadth (1.5-2 cm) above the brow crease. [2, 4]
Temple recession is more variable in the normal adult hairline so there is significant flexibility in designing this area. As a general rule, if a hair transplant patient wants to wear his hair combed straight back, a hairline with more temporal recession will give a denser, fuller look. With side-to-side grooming, a broad hairline will look fuller. (Figures 12 and 13).
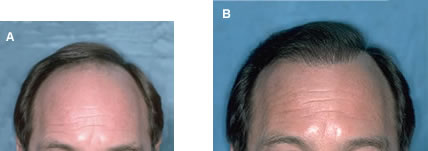 Figure 12. (A) Before and (B) After, in a patient who combs his hair back. High density was achieved in two hair restoration sessions by keeping the frontal area relatively narrow.
Figure 12. (A) Before and (B) After, in a patient who combs his hair back. High density was achieved in two hair restoration sessions by keeping the frontal area relatively narrow.
 Figure 13. (A) Before and (B) After, in a patient who combs his from left to right. High density was achieved in two sessions by taking advantage of side-to-side layering.
Figure 13. (A) Before and (B) After, in a patient who combs his from left to right. High density was achieved in two sessions by taking advantage of side-to-side layering.The key to producing a natural hairline is to create an irregular saw-tooth, or zigzag pattern, at the leading edge. It is more common to error by making the hairline too uniform than by making it too irregular. Besides being irregular, a hairline should also be slightly asymmetric. The hair transplant will look most natural if one side is shaped, and positioned, slightly different than the other. As a very general rule in choosing which side to make lower, it is often best to make the part side slightly lower than the contralateral side. Particular attention should be paid to facial asymmetry as this will often influence the position of the hairline.
Transition zones must be created wherever the edge of the transplanted area is visible. This occurs at the frontal hairline, in the crown, and in the part area on the sides of the scalp. In a typical surgical hair restoration procedure, approximately 200-250 one-hair follicular units are used for the front edge of the hairline. This is immediately followed by two-hair follicular unit grafts. The three- and four-hair units are concentrated in the forelock area, but should extend lateral and posterior in patients with higher density. In all locations, one- and two-hair follicular units should be placed peripheral to the larger grafts to insure a soft, natural appearance.
Hair Direction
Particular attention should be paid to the angle of the recipient sites, since this will determine the ultimate direction that the hair will grow. Hair should be placed into the scalp at the angle it originally grew, not in the direction that it is to be groomed. In general, hair anterior to the vertex transition point should point forward, with the angle of the hair (with respect to the surface the scalp) becoming more acute as one approaches the anterior hairline. At the frontal hairline, the emergent hair is essentially horizontal to the ground (regardless of the slope of the forehead). The direction of hair in the frontal hairline continues to point forward until it approaches the temples where it abruptly changes to a downward anterior and then, at the apex of the temples, to a downward posterior direction. (Figure 14).
Two common mistakes are to transplant the hair radially at the hairline, rather than forward and to follow the direction of a lick or swirl that would otherwise disappear as the patient continued to bald.
 Figure 14. (A) Hair should point forward from one fronto-temporal angle to the other. (B) At the frontal hairline, the angle of the emergent hair is parallel to the ground.
Figure 14. (A) Hair should point forward from one fronto-temporal angle to the other. (B) At the frontal hairline, the angle of the emergent hair is parallel to the ground.Hair should point forward until it reaches the vertex transition point, the area in the posterior aspect of the scalp where the horizontal and vertical planes meet. At this point, the hair changes direction from a predominantly anterior to a radial direction, forming the crown whorl. This point is important in that it represents a natural stopping point for the hair transplant when the donor reserves are limited.20,21
Distribution
The area of the scalp subject to androgenetic alopecia can be divided into three regions: 1) the frontal hairline and frontal scalp, 2) the top or mid-scalp and 3) the vertex or crown. The vertex transition point separates the top of the scalp from the crown.20 (Figure 5.) Since the frontal area of the scalp provides the greatest cosmetic impact, this area should have the greatest hair density. This can be accomplished by placing recipient sites in this area closer together (forward weighting).4 Greater density can also be achieved by placing larger follicular units, i.e. those containing 3- and 4 hairs, in the forward/central part of the scalp (the forelock region). The larger units should not be used at the hairline, so that this zone will remain soft and natural, and they should not be evenly distributed across the scalp, as this will produce a diffuse rather than patterned look. The density should gradually decrease towards the crown. Figure 15 illustrates the overlapping distribution of forward weighting and the forelock zone of central density created by larger follicular unit grafts.8

 Figure 15. The area of forward weighting, created by placing recipient sites closer together, is indicated by the darkened semi-circle. The zone of central density, created by using larger follicular unit grafts, is indicated by the dark egg-shaped region.
Figure 15. The area of forward weighting, created by placing recipient sites closer together, is indicated by the darkened semi-circle. The zone of central density, created by using larger follicular unit grafts, is indicated by the dark egg-shaped region.Most hair restoration patients have enough donor hair to allow the surgeon to extend the transplant to the vertex transition point. As mentioned, this is a natural stopping point since, even if the crown continues to enlarge, transplants performed to this point will maintain a natural appearance, even without additional surgery. Hair transplants should be extended past the vertex transition point into the crown only when the doctor is relatively certain that there will be an adequate donor supply to create a swirl and follow the hair loss laterally if the balding progresses. The indications for transplanting the crown depend upon a number of additional factors and are detailed in reference 3.
Although the transplanted hair direction should not be based upon the way a person intends to groom his or her hair, there are other aspects of transplant design that should be influenced by hair styling preferences, if this is known in advance of the procedure. The degree of temple recession has already been mentioned. Another decision is graft weighting.
In general, the grafts should be forward weighted in the anterior-posterior direction, and symmetrically distributed from left to right. However if a hair restoration patient is relatively certain that they will comb their hair to the side, or diagonally backwards, then hair may be weighted on the part side to give the appearance of greater fullness. This may be accomplished by creating recipient sites more closely together on the part side, by placing larger follicular units in this area, or by doing both. When using larger follicular units, it is important to still create a soft transition zone of one and two-hair units at the visible edge of the part.
It is difficult for patients, particularly those who are extensively bald, to know how they will comb their hair after the transplant. Because of this, it is best to transplant the first session in a symmetrical pattern. However, once the session has grown in, if they are relatively certain that they will continue to groom their hair in one specific way, subsequent sessions can be weighted to one side for greater fullness. Transplanting the first session symmetrically will help insure that there are no gaps in the distribution and that the weighting will not be at the expense of a natural look. (Figure 16).
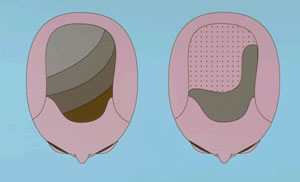
 Figure 16. Side weighting. The figure on the left, illustrates a gradual diagonal side-weighting of the larger grafts on the part-side (darkest area). The figure on the right shows side-weighting in the extreme where hair is concentrated at the frontal hairline and part-side. The remainder of the scalp has scattered follicular units called “tacking hairs” as they are used to hold down the hair from the frontal hairline and part side combed back over this area.
Figure 16. Side weighting. The figure on the left, illustrates a gradual diagonal side-weighting of the larger grafts on the part-side (darkest area). The figure on the right shows side-weighting in the extreme where hair is concentrated at the frontal hairline and part-side. The remainder of the scalp has scattered follicular units called “tacking hairs” as they are used to hold down the hair from the frontal hairline and part side combed back over this area.Regular vs. Dense Packing
It is generally accepted that transplanting up to 25 follicular units per cm2 will not impede their growth. Although there are few well controlled studies addressing the issue, many practitioners feel that “dense packing,” as defined by densities above 25 follicular unit/cm2 grafts, may risk graft survival when performed in large hair transplant sessions and in certain patients. Until there are good scientific studies to clarify this issue, it is probably prudent to consider the following:
- There is probably significant patient-to-patient variability in the ability to support grafts that are densely packed.
- Significant solar damage, which alters the cutaneous vasculature, is a relative contraindication to dense packing.
- Densely packed grafts are more difficult to place and have a greater risk of popping than more generously spaced grafts.
- Dense packing should be considered when the majority of follicular unit grafts can fit into recipient site wounds no greater than those made with the equivalent of a 19-g hypodermic needle.
- Dense packing is often performed by trimming grafts very closely and breaking up naturally occurring 4- and sometimes 3-hair follicular units.
- The additional density achieved with very dense packing may come at the expense of graft survival.
One should consider that the average non-balding scalp has 100 follicular units per cm2 and that approximately 50% may be lost before there is any noticeable thinning. It would be wasteful, therefore, for more than 50% to be replaced – especially since hair transplants are always performed in the face of a limited donor supply. If the larger three- and four-hair units are placed in select areas, more than 25% of the initial density can be achieved in one pass of 25 follicular unit/cm2. With two procedures this density can be achieved in many hair restoration patients.8
Some physicians advocate a “one-pass” procedure to achieve the final density in one treatment session.34 Although this may be appropriate for some patients, the increased incidence of graft popping, desiccation, insertion injury and possible vascular compromise, may lead to poor growth. For very bald patients, very dense packing may not permit coverage of an entire bald area unless very large numbers of grafts are used. Until good scientific studies demonstrate that dense packing in very large hair transplant sessions will allow optimal growth in the majority of patients, covering the entire bald area with moderate density and then increasing density in a subsequent session may be a more judicious strategy, as this allows a natural distribution to be created in the first procedure and it avoids the potential risks associated with very dense packing or extremely large sessions.
Coronal (Horizontal) vs. Sagittal (Vertical) Incisions
Follicular units emerge from the scalp in either a bundle or in a linear array. When in a linear configuration, the orientation is generally in a coronal (horizontal) plane, allowing the follicular units to shingle and provide more coverage than if they were sagittal or random. It has been argued that during a hair transplant there is less scar contraction with a coronal incision compared to a sagittal one. This would allow follicular units to remain linear after they have been transplanted and provide the rational for using coronally angled grafting (CAG) to best approximate the way hair grows in nature.36
The main advantage of CAG is that it would provide a fuller look to the transplant compared to traditional (sagittal) incisions. Another advantage is that grafts may be positioned at a more acute angle with the surface of the scalp and there may be less tendency of the growing hair to elevate in the vertical plane. This is particularly important at the temple/sideburn area where the hair lies very flat to the scalp surface. It is also felt by some practitioners that CAG exhibits less popping and that the wounds cause less damage to the vascular bed.
Hair restoration doctors using sagittally angled grafts (SAG) feel that the pre-made vertical recipient sites are easier to see and that grafts are easier to place in these sites, minimizing injury to the follicular unit grafts. This may be particularly relevant in areas where there are significant amounts of hair present and the hair transplant surgeon does not have the luxury of shaving the scalp before the procedure. It has also been pointed out that coronal incisions (which cross Langer’s lines) potentially cause more damage to collagen and the cutaneous vasculature, than sagittal incisions. An additional concern is that, although there is possibly more hair elevation with sagittal than coronal incisions, there is less lateral (radial) splay of hair when the former is used. Al with minimizing lift, minimizing lateral splay is also an issue of significant cosmetic importance. Finally, if one considers that many follicular units are not linear and that many linear units may indeed contract during the healing process and lose their linear orientation, CAG may offer only a theoretical advantage.36-38
At the time of this writing, there is no consensus on which method is best and if the differences are even significant for most patients, although there is a general trend towards CAG. As with many techniques used in surgical hair restoration, the advantage of one over the other may ultimately depend upon the particular patient, a particular transplant session, or the skills and preferences of a particular surgeon. A number of researchers are currently examining these issues; however, regardless of the outcome, considering the rotational orientation of follicular unit graft adds an important new dimension to follicular unit hair transplantation. (Figures 17 and 18)
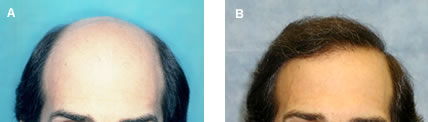

Figure 17. (A) Before and (B) After three sessions in a Norwood Class 6/7 patient with straight, medium-fine, dark hair and light skin. Sagital slits were used in this patient.

 Figure 18. (A) Before and (B) After two sessions in a Norwood Class 6/7 patient with slightly wavy fine, blond hair and light skin. Note how recipient site factors caused the patient’s original wave to return. Sagital slits were used in this patient.
Figure 18. (A) Before and (B) After two sessions in a Norwood Class 6/7 patient with slightly wavy fine, blond hair and light skin. Note how recipient site factors caused the patient’s original wave to return. Sagital slits were used in this patient.


