
Pages:
&after=
&link_before=&link_after=‘); ?>
Optimizing Outcomes
Transition Zones
A soft, natural hairline is the hallmark of an optimal hair transplant. However, careful observation of a normal frontal hairline reveals that there is no actual “line,” but rather an irregular, slightly asymmetric “transition zone” or gradation of follicular units of increasing size and density. This is what should be replicated during a surgical hair restoration procedure (Fig. 34.23a-b). Transition zones are not limited to the frontal hairline; they must be re-created wherever the edge of the transplanted area is visible. In Figure 34.23d, one notes that transition zones have been created at the frontal hairline, sides and vertex transition point leading to the crown.
Although there are an infinite number of ways to create a transition zone at the frontal hairline during a hair transplant procedure, the placement of approximately 50-100 single follicular units in front of a band of staggered single units, one to three rows deep, will usually achieve the appropriate softness. This should be followed by two-, three- and eventually four-hair units, but the larger units should be more centrally located (Fig. 34.23C). With finer hair, larger units may be placed closer to the hairline. It is important to limit the depth of the single hair units, or the zone will appear too thin.
Visibility
Pre-making all the recipient sites prior to graft insertion helps to control bleeding during the hair transplantation procedure and limits the need for epinephrine (adrenaline) (Fig. 34.23D). It initiates the “extrinsic pathway” so that coagulation can begin before the grafts are introduced and allows for easy cleaning of the recipient area of any blood or coagulum, without the risk of dislodging grafts. It also makes it possible to place sites close together without a concern for grafts in adjacent sites from popping. Most importantly, it provides maximum visibility in placing phase of the procedure.46
If the initial sites are scattered, they tend to cause the cutaneous vasculature of the scalp to “clamp down,” increasing visibility for subsequent passes and allowing the skipped areas to be filled in. When pre-making sites, the logistics of matching the number of sites to the number of grafts can be solved by making “projections” of the anticipated number of grafts while the dissection is still in progress.
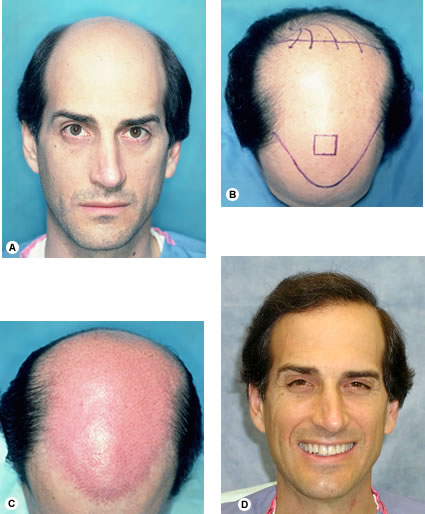 Fig. 34.23. (A) Pre-op. (B) Pre-op markings of the planned procedure. (C) First session just prior to placement, showing the distribution of 2355 recipient sites (D) One year after two hair restoration sessions totaling 4295 follicular unit grafts.
Fig. 34.23. (A) Pre-op. (B) Pre-op markings of the planned procedure. (C) First session just prior to placement, showing the distribution of 2355 recipient sites (D) One year after two hair restoration sessions totaling 4295 follicular unit grafts.Recipient Site Influences
Some hair characteristics, such as waviness, are governed by the recipient site. When individual follicular units are placed into very small wounds, there is little fibrotic reaction to the grafts and the recipient area can exert its influences on hair growth. In Figure 34.24, note the delicate wave produced by the recipient scalp. Because the cylindrical shape of the follicular unit gives no clue as to its orientation, it would be impossible for the hair transplant surgeon to intentionally rotate the hair to product this effect.

 Fig. 34.24 (A) Pre-op, Norwood Class VI, with very fine, blonde hair and a donor density of 2.5 hair/mm 2. (B) One year after two sessions of 2678 and 1836 follicular unit grafts.
Fig. 34.24 (A) Pre-op, Norwood Class VI, with very fine, blonde hair and a donor density of 2.5 hair/mm 2. (B) One year after two sessions of 2678 and 1836 follicular unit grafts.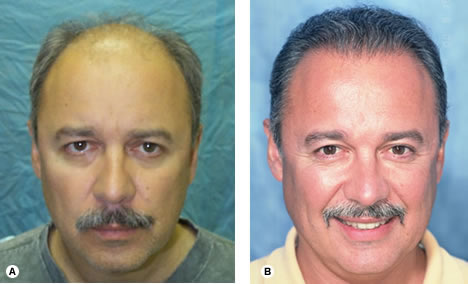
 Fig. 34.25 (A) Pre-op of Early Norwood Class VI. (B) One year after one session of 2520 follicular unit grafts.
Fig. 34.25 (A) Pre-op of Early Norwood Class VI. (B) One year after one session of 2520 follicular unit grafts.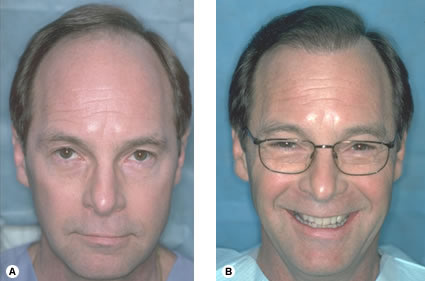
 Fig. 34.26 (A) Pre-op, Early Norwood Class V. (B) One year following two sessions of 2105 and 1665 follicular unit grafts.
Fig. 34.26 (A) Pre-op, Early Norwood Class V. (B) One year following two sessions of 2105 and 1665 follicular unit grafts.
 Fig. 34.27 (A) Pre-op, Norwood Class V. (B) Integrating hair with a persistent frontal forelock (one year following two sessions of 2133 and 1,171 follicular unit grafts.)
Fig. 34.27 (A) Pre-op, Norwood Class V. (B) Integrating hair with a persistent frontal forelock (one year following two sessions of 2133 and 1,171 follicular unit grafts.)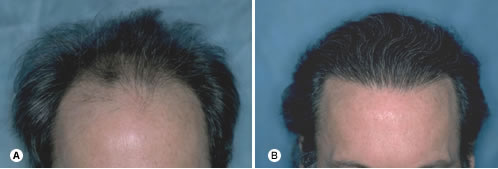
 Fig. 34.28 (A) Pre-op of 46-year-old early Norwood Class IVA with wavy, medium-coarse hair. (B) Post-op after two sessions of 2085 and 1438 follicular unit grafts.
Fig. 34.28 (A) Pre-op of 46-year-old early Norwood Class IVA with wavy, medium-coarse hair. (B) Post-op after two sessions of 2085 and 1438 follicular unit grafts.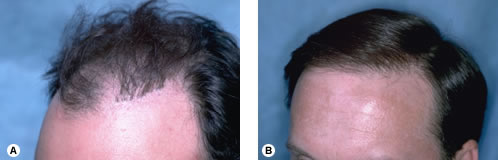
 Fig. 34.29 (A) Pre-op showing large grafts forming a literal wall of plugs. (B) Camouflage from one session of 1818 follicular units.
Fig. 34.29 (A) Pre-op showing large grafts forming a literal wall of plugs. (B) Camouflage from one session of 1818 follicular units.Hair Direction
When the hair is planted at the frontal hairline in its natural forward-pointing direction, combing it back causes it to bow, giving it the appearance of fullness. A common mistake is to point the hair in the direction that the patient plans to comb their hair; this makes the hair lie flat and bodiless when groomed. On the other hand, as the frontal hairline approaches the temples, the hair direction should be abruptly changed, so that it is angled downward and lying very flat on the scalp. Perfect integration of the frontal hairline with hair on the sides and temples is essential if the hair restoration is to look completely natural (Fig. 34-25).
Hairline Placement
If it is to look natural throughout the patient’s life, the hairline created during hair transplantation must simulate that of a mature adult. In the adolescent male, the frontal hairline touches the top crease of the brow when the eyebrows are raised (i.e. the hair begins at the upper border of the frontalis muscle). In a mature adult, the mid-portion of the frontal hairline rests approximately one finger-breadth (1.5-2 cm) above the brow crease. Although the degree of temple recession can vary dramatically in the normal adult hairline, the mid-part of the frontal hairline is crucial in framing the face.1,8 Significant bitemporal recession was built into the restoration of the hair transplant patient in Figure 34.26, yet the forward-placed mid-portion sets his facial features in the correct proportions.
Forelock Integration
A persistent frontal forelock poses an interesting dilemma. When hair is transplanted around the forelock, the patient may be left with a gap in his frontal hairline if the forelock eventually disappears. On the other hand, it is wasteful to add hair to a forelock with adequate density that may persist for years. The solution is to check for miniaturization with a densitometer. The patient in Figure 34.27 had miniaturization in his forelock greater than 50%, suggesting that it would not be stable over time. Two surgical hair restoration sessions were used to integrate transplanted hair into the resident terminal hair of the forelock, producing a central density that should persist for many years.
Optimizing Density
One of the beauties of Follicular Unit Hair Transplantation is the ability to sort the three- and four-hair units and place them in the forelock area, creating a density significantly greater than if the grafts were evenly distributed. This is possible because the compactness of the follicular unit allows four-hair grafts to be placed into very small sites.6,8 In certain instances, follicular units may contain more than four hairs, and adjacent follicular units are occasionally so close together that they can fit into a small recipient site.62,63 However, as long as these “grouped grafts” are placed in a central location and the recipient wounds are kept small, this technique can add density without risking an unnatural look. It is important to keep in mind that ultimate density depends on the absolute number of hairs moved rather than the size of the grafts.64 Using grafts larger than follicular units always risks that the hair transplant surgery may look unnatural. The patient in Figure 34.28. achieved a very dramatic frontal density in two sessions using the technique of follicular unit sorting.
Creating Camouflage
A sizable part of many surgical hair restoration practices involves repairing transplants performed with older techniques. FUT is ideal for this because of follicular units’ small size and high hair count.65,66 Often fixing a pluggy look requires graft excision (with reimplantation) prior to the actual hair transplant. However, the patient in Figure 34.29. had a row of plugs set far enough back from his frontal hairline that camouflage with follicular units alone was sufficient for the repair.
Automation
Short of cloning follicular units in a Petri dish, the future in Follicular Unit Hair Transplantation optimization lies in the development of automated devices that can harvest the donor strip, isolate individual follicular units, create recipient sites and insert grafts–all without the risk of human variability or error. A number of creative instruments have been designed toward this end, but thus far their success has been limited.67-70 Much of the difficulty lies in the inherent variability of the human scalp and the follicular unit itself. The full automation of a hair restoration procedure that is labor intensive, organizationally complex and dependent on the aesthetic judgment of the hair transplant surgeon remains a formidable challenge.
Postoperative Care
Patients are called at home the day after the procedure and seen in our office one week post-op. They come in again 10 months later to assess growth, have their pictures taken and discuss the possibility of additional surgery. Those with questions or concerns are seen as frequently as needed. Table 34.12 summarizes typical post-op instructions.
Table 34.12 Summary of Post-Op Instructions Following Follicular Unit Transplantation
Care of Transplanted Area
Shampoo every three to four hours the day following the hair restoration procedure, and then twice daily until your one-week post-op visit. Be especially careful when cleaning the transplanted site in the first few days so that the grafts will not be dislodged. However, a thorough but gentle rinsing of the recipient area will minimize crusting and make the hair transplantation less noticeable. When shampooing and rinsing the transplanted area, be gentle for the first two weeks following the hair transplant surgery. Do not rub, pick or scratch, as this may dislodge grafts.
Care of Sutured Area and Non-Transplanted Parts of Scalp
Gently wash the sutured area with your fingertips using copper peptide containing shampoo. Shower water may hit the sutured area in the back of your scalp directly. You may use a hair dryer set on warm, but not hot. Do not use any scalp or hair coloring agents for at least two weeks after your procedure.
Post-Op Medications
After your procedure, you will be given sleeping medication, pain pills and medication for hiccups.
Itching
You may experience some itching either in the transplanted area or sutured area following your surgical hair restoration procedure. Hydrocortisone ointment may be applied locally to the areas that itch as needed, up to four times a day.
Swelling
You will be given an injection of cortisone during your procedure to decrease swelling after surgery. If there is significant swelling, it usually occurs around the second to fifth day post-op and should not be cause for concern. It resolves by itself after a few days and does not require any special treatment. Cool, wet dressings may be placed over the swollen area, but make sure they do not touch the grafts.
Bleeding
Before you leave the office, all bleeding will be controlled. Rarely some bleeding may occur after the hair transplant. If this happens, apply firm, continuous pressure on the area. If you are unable to contact us through our pager, go to the nearest emergency room and show our instructions to the physician on duty.
Exercise, alcohol, smoking and other restrictions
Avoid direct trauma to the head for two weeks after the procedure, and abstain from sexual intercourse, alcohol use and smoking for three days after the procedure. After two weeks, you may resume your normal daily activities.
Sun
Avoid unprotected exposure to sunlight for three months. Wear a hat when you are going to be outside or use a strong sunscreen with a SPF of 30+.
Infection
Redness, swelling and slight tenderness are to be expected for the first few days after a hair restoration procedure. Persistent swelling, pain or tenderness in the sutured area may be a sign of infection. Fever and/or chills are indications of infection as well. There also may be a discharge or puss in the suture line. If any of these conditions should occur, please contact the office.
Numbness
Scalp numbness, tingling or similar sensations may occur temporarily. This generally disappears within a few weeks to months, as nerve endings regrow.
Hair-Loss Medications
Minoxidil 5%: If you plan to continue this medication, resume it one to two weeks after the hair transplant surgery.
Finasteride 1mg: This medication should not be discontinued for the procedure.
Pages:
&after=
&link_before=&link_after=‘); ?>


