
Pages:
&after=
&link_before=&link_after=‘); ?>
Preoperative Preparation
Patient Evaluation and Surgical Planning
Diagnosis and Classification of Androgenetic Alopecia
The diagnosis of androgenetic alopecia in men is generally straightforward. It is made by observing a “patterned” distribution of hair loss and confirmed by the presence of miniaturized hairs in the areas of thinning. The diagnosis is supported by both the inexorable progression of the hair loss according to a recognizable pattern and a history of baldness in the family.27 In women, the diagnosis is more complex, as the most common presentation, a diffuse pattern, can be mimicked by a host of non-androgenetic etiologies.
Miniaturization — the progressive diminution of the hair shaft’s diameter and length in response to androgens — can be most readily observed with a densitometer,12 a hand-held instrument that magnifies a small area of the scalp where the hair has been clipped to about 1 mm. One type, the Rassman densitometer,4 magnifies by 30x in a visual field of 10mm2, making it easy to spot miniaturization and calculate hair density. (Figs 34.1 – 34.3)
When describing hair loss, particularly in the early phases, it is preferable to think in terms of changes in volume rather than density. Density is simply the number of hairs per unit area, whereas volume reflects both hair shaft diameter as well as the absolute numbers of hairs.28 The earliest signs of hair loss, that of miniaturization, result in volume changes caused by the individual hair decreasing in size without a decrease in their number. Only in more advanced balding will the actual number of hairs start to decrease.1
The Norwood classification of male hair loss, published in 1975, remains the most widely used.29 It defines two major patterns and several less common types (fig.34.4). In the regular Norwood pattern, two areas of hair loss–a bitemporal recession and thinning crown–gradually enlarge and coalesce until the entire front, top and crown (vertex) of the scalp are bald.
 Fig. 34.1 Hair Densitometer.
Fig. 34.1 Hair Densitometer.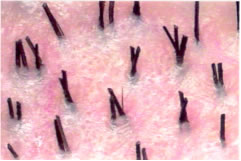
 Fig. 34.2 Natural hair groupings as seen through a densitometer (magnification x 30).
Fig. 34.2 Natural hair groupings as seen through a densitometer (magnification x 30).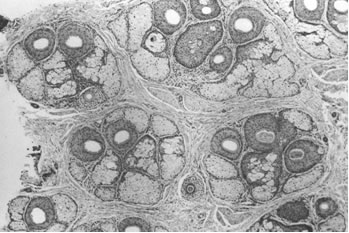
 Fig. 34.3 Histological view of follicular units corresponding to the natural hair groups observed on the scalp surface. Transverse section taken at the level of sebaceous glands (hematoxylin and eosin, original magnification x 40).6
Fig. 34.3 Histological view of follicular units corresponding to the natural hair groups observed on the scalp surface. Transverse section taken at the level of sebaceous glands (hematoxylin and eosin, original magnification x 40).6The less common pattern, Norwood Class A, is characterized by a distinctly anterior to posterior progression usually resulting in baldness on the front and top of the scalp, but more limited loss in the crown. In both patterns, the sides and back tend to resist androgenetic changes, though the sides may exhibit significant thinning in senile alopecia.
Two other types of genetic hair loss not emphasized in the literature, Diffuse Patterned and Diffuse Unpatterned Alopecia, pose the greatest challenge both for diagnosis and patient management. A thorough familiarity with all of these patterns is essential for diagnosing androgenetic alopecia and planning Follicular Unit Hair Transplantation.
Table 34.1 Classification of Androgenetic Alopecia
- Norwood Classes
- Regular Norwood Classes I to VII
- Type A Variant (IIa to Va)
- Variations:
- persistent frontal forelock
- persistent frontal hairline
- Diffuse Androgenic Alopecias
Diffuse Patterned Alopecia (DPA)
Diffuse Unpatterned Alopecia (DUPA) - Senile Alopecia
Diffuse Patterned Alopecia (DPA) is an androgenetic alopecia manifested as diffuse thinning in the front, top and vertex, with a stable permanent zone. In DPA, the entire top of the scalp gradually miniaturizes without passing through the typical Norwood stages. Diffuse Unpatterned Alopecia (DUPA) is also androgenetic but lacks a stable permanent zone and affects men much less often than DPA.

 Fig. 34.4 Norwood Classification.28
Fig. 34.4 Norwood Classification.28DUPA tends to advance faster than DPA and eventuate in a horseshoe pattern resembling the Norwood class VII. However, unlike the Norwood VII, the DUPA horseshoe can look almost transparent due to the low density of the back and sides. Differentiating between DPA and DUPA is very important because DPA patients often make good hair transplant candidates whereas DUPA patients almost never do, as they inevitably suffer extensive hair loss without a stable zone for harvesting.7
There are five early signs of DUPA:
- A rapid decrease in hair volume (as distinguished from density) and a change in hair texture at an early age, often in the teens.
- The maintenance of an adolescent hair pattern and persistent frontal hairline in spite of dramatic volume change.
- A see-through donor area, which is greatly accentuated when the hair is lifted up.
- Significant miniaturization of the donor area (>35%).
- A donor density < 1.5 hairs/mm2. (Densitometry’s acute sensitivity in detecting early DUPA certainly justifies its routine use in the evaluation of hair loss.)
If a diagnosis of DUPA is even remotely suspected, any decisions regarding surgical hair restoration should be postponed. The possibility of missing a DUPA diagnosis is one of the most powerful arguments against performing hair transplantation at an early age.
Both DPA and DUPA occur in women; but, in contrast to men, DUPA proves far more common. As with men, female DUPA patients do not make good hair transplant candidates (except possibly when donor hair is used solely to soften the frontal edge of a wig). Indeed, the higher DUPA incidence in women explains why a smaller proportion of women than men qualify as surgical hair restoration candidates. Interestingly, the most common classification used for women, the Ludwig Classification, does not differentiate between DPA and DUPA.30
It is important to emphasize that since a wide variety of medical conditions can produce diffuse hair loss, a non-androgenetic differential must be considered in all unpatterned alopecias. This is particularly relevant in evaluating women in whom unpatterned hair loss is the rule rather than exception (Table 34.2). The following laboratory tests are often useful when a non-androgenetic cause for diffuse hair loss is suspected: chemistry screen, complete blood count, serum iron, total ion-binding capacity, triiodothyronine, thyroxine, thyroid-stimulating hormone, antinuclear antibody and serologic test for syphilis.
Table 34.2 Non-Androgenetic Causes of Diffuse Hair Loss in Women
- Anemia
- Endocrine diseases (esp. thyroid)
- Connective tissue disease
- Obstetric/Gynecologic conditions (e.g. postpartum, polycystic ovarian disease)
- Weight loss (esp. crash diets)
- Emotional and physical stress (e.g. surgery, anesthesia)
- Medications: oral contraceptives, thyroid drugs, antihypertensives (esp. ?-blockers), psychotropics, anticoagulants, antilipemics, gout therapy, prednisone, excessive Vitamin A or tryptophan use
In women, diffuse or patterned hair loss may be a sign of excessive androgen production. A further medical evaluation is indicated when the hair loss is associated with any of the following: cystic acne, irregular menses, hirsuitism, virilization, infertility or galactorrahea. Serum levels of DHEA-Sulfate, androstenedione, total and free testosterone and prolactin levels can serve as a useful screen.31
When the diagnosis of androgenetic alopecia is uncertain, further diagnostic information can be gleaned from a hair-pull test for telogen effluvium, a potassium hydroxide mount and culture for fungus, a microscopic examination of the hair bulb and shaft, and a scalp biopsy (sectioned horizontally).32 But a dermatologic consultation is warranted whenever the diagnosis of hair loss is unclear.
Who is a Candidate for Hair Transplantation?
In all cosmetic procedures, a successful outcome depends on proper patient selection (Table 34.3). In surgical hair restoration, proper timing is also crucial. The only reason for performing a transplant sooner rather than later is for its cosmetic benefit; there are no medical or surgical advantages to transplanting at an early age. The popular rationale that hair transplants should be performed at a young age so that “no one will notice” does not make sense: If there is nothing to notice after the hair transplant matures, why perform it in the first place? FUTs heal so quickly and the hair growth is so gradual that, once the short post-op period ends, the process is almost always undetectable.
Table 34.3. Patient Selection in the Surgical Treatment of Androgenetic Alopecia
Age: 23-25 years or older
Inadequate response to medication after one year
Significant hair loss: Norwood Class III or greater
Diffuse patterned alopecia (DUPA) has been ruled out
Non-androgenetic causes of hair loss have been ruled out*
No medical contraindications to surgery (e.g. drug sensitivities, keloids, connective tissue disease†)
Reasonable patient expectations
* Many non-androgenetic causes of hair loss can be treated with hair transplantation
† Some are relative contraindications
Patients seeking hair transplant surgery while still in their early twenties invariably wish to have their adolescent hairline and original density restored. Since neither of these goals can be achieved surgically without compromising the patient’s future appearance, the procedure should not be performed at his age. It should be explained that hair transplantation is a procedure that moves, rather than creates, new hair, so that it can never increase overall hair volume. And, in the face of decreasing total volume over time, the pattern of the transplanted hair must take into account this decreased total hair mass. In other words, patients who will have significant balding need to have built-in temporal recession and possibly a crown that is significantly thinner than the surrounding hair for the transplant to look natural over time. Unfortunately, neither of these is generally acceptable to a young man in his early twenties.
Another reason to postpone hair transplants for those under 25 or with only limited hair loss is to give medications–particularly finasteride–adequate time to work. Since patients may continue to show regrowth for up to two years after treatment is initiated, they should in general take finasteride at least this long before surgery is considered. It is inappropriate, therefore, to start younger patients on finasteride and schedule surgery at the same time. Fortunately, finasteride works best in younger hair restoration patients and especially those with large areas of miniaturized scalp rather than areas that are totally bald. On the other hand, for older patients who would be taking finasteride to maintain rather than regrow hair, and for those whose advanced state of hair loss makes results from finasteride unlikely, the medication may be prescribed concomitantly with hair transplant surgery scheduling (see “Preoperative Preparation”).
With the availability of finasteride, medication plays an increasingly important role in the management of androgenetic hair loss. Although the incidence is small (2%), the stigma of possible sexual side effects has turned many against this drug. Many also consider surgery a more conservative form of treatment than the potential lifetime use of a drug. Because of these concerns, and the often palpable desire of panicked patients to rush to surgery, the physician should take time to thoroughly discuss the pros and cons of medical therapy in all patients.
In the Norwood Classification, Class I represents a normal adolescent pattern and Class II a normal non-balding adult. Therefore, at minimum patients should qualify as Class III before hair transplants are contemplated. Early Class III patients will often benefit from medication alone, so this should be considered first. On the other end of the spectrum, extensive balding need not make a patient unsuitable for surgery, so long as the donor zone is stable (miniaturization < 20%) and the patient's expectations are commensurate with his or her available donor supply. As long as the patient is in good health, there is no upper age limit. In fact, older patients tend to have the most reasonable expectations and often make the best candidates. There are few absolute medical contraindications to surgical hair restoration, particularly since it is an outpatient procedure not requiring general anesthesia. Relative contraindications include: bleeding disorders, immunodeficiency, unstable arrhythmias, COPD, sensitivity to local anesthetics or adrenaline, a history of keloid formation or connective tissue disease and major psychiatric disorders. When in doubt about patients' medical condition, it is always best to get medical clearance from their primary physician. Patients should be able to tolerate being in the surgical chair a good part of the day; consequently, back and neck problems as well as claustrophobia can sometimes make the procedure problematic. Special care should be taken when evaluating patients with significant psychiatric problems, particularly depression; in such cases, a psychiatrist or psychologist should participate in the decision-making process. Possibly the most difficult part of the consultation is managing patients' expectations. It is almost a cliché to say that they must have "reasonable expectations," but ensuring this is the essence of the evaluation. The hair transplant surgeon cannot stress strongly enough that, since transplants move rather than create hair, the resulting density will be significantly less than in the original site. It is also important to emphasize that it is the patient's own hair, from the sides and back of his or her head, that will be transplanted. And the final result can be best described with reference to the texture, color, curl and other qualities of the patient's existing hair. But in addition to a thorough discussion, it is also helpful to provide prospective patients with printed material and photos and to make past patients available for them to meet. Assessing the Patient’s Donor Supply
The main factors in determining total donor reserves are donor density, scalp laxity and size of the donor area.
Donor Density
The number of follicular units in the mid-portion of the donor area of a normal Caucasian male who has not had hair restoration surgery is approximately one per mm2.8 In the first procedure, therefore, the donor area should yield approximately one follicular graft per mm2 of scalp, provided there is no significant wastage during surgery. The average yield declines when longer strips are taken since density decreases towards the sides. In some individuals, density varies dramatically throughout the donor area, but this is the exception rather than the rule.
Since the number of follicular units per unit area stays relatively constant, donor density is an indication of the average number of hairs per graft. For example, if a hair transplant patient has a density of two hairs per mm2, the donor area will generally contain one follicular unit per mm2 and the grafts will consist of a combination of one-, two- and three-hair units, with the average being two hairs per graft. With a density of 2.3 hairs per mm2, there will still be one follicular unit per mm2, so the same number of grafts will be harvested per unit donor area, but the grafts will have an average of 2.3 hairs per mm2 and consist of a mix of fewer one-hair units and a larger percentage of three- and four-hair units.8
Follicular unit density varies according to race, thus the number of grafts obtained per unit area of donor tissue will also exhibit racial variability and must be accounted for in the surgical planning.8
If the scalp has been stretched from previous hair transplants, scalp reductions or scalp lifts, the follicular units will be spaced further apart, making it necessary to actually measure the density of follicular units to accurately estimate the number of grafts obtainable from the strip (as the density of follicular units will now be less than 1/mm2).
Donor scarring from previous surgeries will also significantly diminish the donor yield. All donor harvests, no matter how perfectly executed, entail some loss of hair. In addition, the angle of the hair surrounding the scar will be altered slightly, creating more transection in any subsequent harvest.
A person can lose a substantial amount of hair volume–either due to actual loss of hair or to miniaturization–before it becomes noticeable. When the hair is blonde or white, it takes longer for thinning to show, while it is evident sooner for those with black hair and white skin. For those with average density and average hair attributes, approximately half of the hair in the donor area may be moved without a significant change in appearance.
Scalp Laxity
Scalp laxity is an important factor in determining total available donor hair. In those with loose scalps, harvesting the donor strip merely removes some scalp redundancy while only slightly affecting density (hairs per mm2). With tight scalps, however, each hair restoration procedure stretches the skin, measurably decreasing density. The limitations of a tight scalp are usually not apparent in the initial surgery, but in subsequent procedures it can become much harder to perform a non-tension closure or, in the face of decreased density, to harvest a significant amount of hair. Therefore, the long-term goals of those with tight scalps must reflect a more limited donor supply.
At the same time, patients with very loose scalps tend to heal with widened scars and so often make poor candidates for procedures using a linear incision. Some, in fact, may have undiagnosed connective tissue disease.33 Follicular unit extraction should be considered in cases of very loose and very tight scalps.2
Donor Dimensions
The mid-portion of the harvestable donor zone generally lies over the occipital protuberance and extends to within 3 cm of the temple hairline on either side. This distance is approximately 32-34 cm. Recession at the temples can signal extensive balding and portends a limited donor supply. The height of the permanent zone can vary markedly from person to person and should be carefully measured. Hair should be harvested only where it is stable, i.e. where it lacks significant miniaturization. An often overlooked sign is the “ascending” hairline, characterized by miniaturization in the lower margin of the permanent zone. Both receding temples and an ascending posterior hairline indicate a shrinking donor zone and mandate conservative surgical planning.
Planning the First Hair Transplant Session
Ideally, the main goals of the first transplant session should be:
1. To establish the frontal hairline and frame the face.
2. To provide coverage to all bald areas of the scalp, from the frontal hairline back to the vertex transition point.34
3. To create sufficient density so that the results will look natural after one session, though additional sessions may be desired.7
These goals may not be achievable with a small or inexperienced surgical team, but should be the ultimate aim of those performing hair restoration surgery. In this author’s opinion, there is little medical or aesthetic justification for performing the surgery in arbitrarily small sessions. It is preferable that each procedure cover the entire area of hair loss intended to be treated and be designed to “stand alone.”7,8
In an alternate approach to surgical planning, the objective is to achieve final density in a one-pass hair transplant procedure by creating high density in smaller area and then transplanting another area in a subsequent session. This is accomplished in part by using very small recipient sites, limiting graft size to three hairs and using the stick-and-place method, in which grafts are inserted as soon as the recipient sites are made.35
As the number of grafts placed per unit area (density) rises, so too does the risk of vascular compromise that may result in sub-optimal graft growth. Technical problems of popping that may cause the grafts to become desiccated or that exposes the grafts to mechanical injury on reinsertion, also becomes more likely. Proper patient selection and technical expertise help avoid such problems, but the risks are increased nevertheless. It certainly behooves those with more limited experience to be conservative in this aspect of the surgical hair restoration procedure.
Because the blood supply to the scalp is extensively collateralized,36 the risk of vascular compromise is related more to the density of grafts in a specific area and the size of the recipient wounds, than the absolute numbers of grafts placed. For this reason, the transplantation of a large number of grafts over a broad area does not seem to pose the same problems as producing very high densities. In addition, popping becomes less of a technical issue when the same number of grafts are placed over a larger area. However, transplanting large number of grafts (in “mega-sessions”) poses its own challenges, such as increasing the time the grafts remain outside the body, requiring more staff, contributing to patient and staff fatigue, and creating organizational issues. As with dense-packing, the use of very large sessions should be reserved for only the most experienced surgical teams.
Though the amount of hair needed to cover the front and top of the patient’s scalp will vary, an attempt should be made to achieve this coverage, if only lightly, in the first session. Crown coverage should not be a goal of the first session unless the patient has an above-average donor supply; if it is attempted in the first session, the patient’s options will be more limited and the chances for an aesthetically balanced transplant may be permanently compromised. Table offers general guidelines as to the number of follicular units needed for the first hair transplant surgery.
Table 34.4 Number of Grafts in First Follicular Unit Transplant Session

Planning a Second Session
Timing of the Second Session
Transplanted hair sheds around two to six weeks after the procedure, and the first signs of new growth occur on average in approximately 10 weeks, though the onset can vary considerably, taking as long as four to six months or more. Hair gradually increases in both thickness and length, so that the initial growth is often not indicative of the final result. In less than 5% of patients, hair grows unabated after hair restoration surgery, skipping the shedding phase.
One should generally wait 8-12 months to best appreciate the cosmetic impact of the procedure. During this time, the continued increase in the hair’s diameter and length strikingly alters the patient’s appearance. Once the hair reaches styling length, both the patient and physician can make aesthetic judgments about the weighting and balance of additional grafts.
It will also be advantageous to delay the second procedure to maximize the donor harvest. Although each hair transplant procedure results in a potentially tighter scalp, some of the preoperative donor laxity returns in the months following the surgery. The major change will occur during the first month as the edema and inflammation subside. However, further loosening will occur as the scalp stretches over the next six to 12 months.
In the uncommon event of telogen effluvium occurring in the donor area, the telogen follicles may not be easily identifiable in the dissection. Since recovery in the donor area may take up to a year, it is essential that hair transplantation patients wait until complete regrowth has taken place before a second session is performed. In rare cases, if the closure is too tight, the effluvium may eventuate in permanent hair loss.
Goals for the Second Session
The main goals of the second hair restoration session are:
1. To add density to areas transplanted in the first session.
2. To refine the hairline.
3. To follow the progression of the hair loss (if necessary).
4. To extend the transplant into the crown (when appropriate).
In general, most patients require two sessions to achieve adequate density. The hairline often can benefit from a little tweaking to make the leading edge softer and more irregular. Placing the hairline too low is a common mistake, but so is placing it too high, something often done with the intention of bringing it down on the second session, once the patient can see how it looks. It is better to get the hairline position right in the first session; lowering it later often leaves the leading edge too thin.
The decision regarding crown coverage is important because it is the least visible of the balding regions, but can potentially occupy a very large surface area, producing an almost inexhaustible demand upon the donor supply.
If extensive balding appears likely and the patient has a modest donor supply, the crown should be treated as an extension of the top, rather than an isolated region, to ensure that the patient will not be short of hair if the intervening bridge between the front and crown were to require additional grafts. Unless the patient’s history, age and physical exam indicate limited balding, it is particularly important to avoid creating high density in the crown, as subsequent balding could leave an isolated island of hair. How much of the crown to cover is a critical decision; though the least visible of the balding regions, it can occupy a very large surface area, generating an almost inexhaustible demand upon the donor supply.
A useful alternative to covering the crown with transplanted hair is to halt the transplant at the vertex transition point.34,37 The patient can then groom the hair back to conceal the non-transplanted area. This is recommended when direct crown coverage is not realistic or it is too early in the balding process to determine whether significant crown coverage will be possible in the future. Another advantage of sparing, or lightly covering, the crown is that donor reserves may be saved to address further diminution of the donor fringe.
Subsequent Transplant Sessions
The hair transplant surgeon should make every attempt to accomplish the restoration in as few sessions as possible, rather than putting patients through an unnecessarily protracted course of multiple surgeries that can mar both their donor area and lifestyle. A second session is especially problematic for actively balding patients, therefore, when hair transplantation patients are experiencing an accelerated phase of hair loss, medical therapy should be encouraged and in general surgery should be postponed.
The number of grafts required to achieve patient satisfaction varies widely due to the great variability in hair characteristics. Moreover, since hair loss patterns form a continuum while the Norwood classes are discrete, even the transplant size necessary for each class can vary significantly. Table shows the approximate number of follicular implants necessary for a complete restoration, without and with crown coverage.
Table 34.5 Total Number of Follicular Unit Grafts for a Complete Restoration

The Patient
Hair restoration doctors commonly place patients on finasteride before surgery to minimize the chance of post-surgical effluvium. Although there are no scientific studies confirming that it is effective in doing this, it would seem that if the goal is to prevent post-surgical shedding, the medication should be prescribed at least several months prior to the procedure. If, however, the intent is to postpone or obviate the need for surgery, then it should be taken for a minimum of one year.
Patients using topical minoxidil are advised to discontinue its use several days before surgery (because of its vasodilator properties) and wait until a week after the procedure before resuming (to avoid the irritating effects of the alcohol in the 2% solution or the propylene glycol in the 5% solution). Although we suggest minoxidil in combination with finasteride for patients with early hair loss, we generally do not recommend its use after a hair transplant, unless it is being used in an area other than that which was transplanted (such as the crown). We feel that minoxidil has little added value for the average post-transplant patient. We do, however, encourage the continued use of finasteride to help retard further balding. Those who do not plan to use minoxidil after surgery should discontinue it immediately, so that any of its beneficial effects may be reversed by the time of surgery.
Patients are advised to avoid products that are used to thicken the hair or stain the scalp for three days prior to the procedure, as these often take several days to wash out of the scalp completely. Their presence during surgery can decrease visibility and make placing more difficult. All hair systems should be removed prior to surgery and be replaced with, or converted to, a clip-on system. The front edge of the piece can be kept in place with a stiffening-rod without the need for glue or tape. However, any form of attachment at or near the frontal hairline risks dislodging grafts. Patients are encouraged to permanently discontinue the system after the procedure, but those who feel the need to use them until their hair grows in should wait at least five days post-op.
Systemic antibiotics are not indicated for clean surgical wounds in healthy patients, so their routine use in hair transplantation is not necessary; however, many hair restoration doctors – perhaps the majority – do routinely use them. Because there are no specific guidelines for antibiotic prophylaxis in hair transplantation for patients with a history of endocarditis or mitral valve prolapse, the decision to use them must be based on the individual patient’s risk factors. This topic is covered in an excellent review by Haas and Grekin.38
The other pre-op instructions are relatively straightforward and will depend to some degree on the preferences of the operating hair transplant surgeon. Patients should be notified well in advance of the procedure date regarding the need to discontinue certain medications, stop smoking and abstain from alcohol prior to surgery. Table is a summary of the main preoperative instructions.
Table 34.6 Preoperative Instructions
• Continue medications currently prescribed by your physician, particularly those for high blood pressure. Those on broad ?-blockers (such as propranolol) should switch to select ?- blockers, as the former may interact with epinephrine. This should be done under a doctor’s supervision.
• Discontinue topical minoxidil and avoid products used to thicken the hair or stain the scalp three days prior to the procedure.
• In order to minimize bleeding, avoid the following prior to your hair transplant surgery: aspirin or other anti-inflammatory medications (one to two weeks), B or E vitamins (one week), or alcoholic beverages (three days). Do not drink coffee or any other caffeinated beverages on the day of your procedure as these substances will increase your sensitivity to medications such as adrenaline.
• Do not smoke tobacco products for at least 24 hours before your procedure and at least one to two weeks after. Smoking will slow down healing and heighten the chances of wound infection and scarring.
• The morning of your procedure, take a bath or shower and wash your hair thoroughly using a surgical scrub (contains 3% chloroxylenol). If possible, leave your hair long in the back and on the sides to cover the sutures.
• Wear clothes that do not need to be pulled on over your head; this will help keep your bandage in place and avoid any damage to your grafts immediately after surgery.
• Eat breakfast the morning of your procedure. If you are scheduled for surgery in the afternoon, have a light lunch before you arrive.
• Because you may be receiving medications during the procedure that can make you drowsy, you cannot drive home following the surgery. If you must drive or take public transportation, please let your hair restoration doctor know ahead of time.
All patients undergoing hair transplantation should be treated with universal precautions. Although there is no consensus on the need to perform routine blood tests before the procedure, the following tests add an additional level of safety:
• complete blood count
• hepatitis B surface antigen and antibody
• hepatitis C antibody
• HIV screen
One should obtain medical clearance for HIV-positive patients to make sure that they are immunocompetent enough to withstand a potential series of procedures. With the hepatitis antigen-positive patient, there is concern about active disease and one should inform the patient’s primary physician of any positive screening. Other tests, such as a platelet count and prothrombin and thromboplastin times are performed only if warranted by the history and physical.
The surgical consent form should be given to patients to read at their leisure well in advance of the procedure and should be signed before any medications that can cause drowsiness or impair judgment have been given. The exact time of signing should be indicated. The major elements of the consent form are listed in Table 34.7.
Table 34.7 Elements of the Consent Form for Hair Transplantation
• Nature of the procedure, with specific reference to its cosmetic nature
• Indications for hair restoration surgery
• Risks: reactions to anesthetics, allergic reactions, sterile folliculitis, infection, cyst formation at graft site, scarring in donor area, hair loss related to the procedure, hair texture changes, failure of transplanted hair to grow, numbness, paresthesias, temporary swelling or bruising
• Benefits
• Alternatives
o Doing nothing
o Change hair styles (e.g. lightening or keeping hair very short)
o Medical therapy
o Another form of surgical hair restoration (e.g. mini-micrografting)
o Wearing a hairpiece
• Results are not guaranteed
• Consent for photograph as part of the medical record
• Caution about driving under the influence of medication
• Statement that the above are understood and all questions have been answered
• Signature of the patient with date and time (prior to the administration of drugs), countersigned by the operating physician and witnessed by a staff member
The morning of the hair transplant surgery, the patient should shower using a chlorhexadine surgical scrub as shampoo. Though it does not sterilize the scalp, the chlorhexadine binds to the stratum corneum, decreasing transient and pathogenic microorganisms and resident skin flora. Caution is advised, as it can be toxic to the middle ear and irritating to the eyes. After showering, the patient should dress in comfortable clothes and wear a button-down shirt.
Pages:
&after=
&link_before=&link_after=‘); ?>


