
Robert M. Bernstein, MD, New York, NY
William R. Rassman, MD, Los Angeles, CA
Dermatologic Surgery 1997 23(9):771-84.
The concept and technique of “follicular transplantation” has been described by these authors in a 1995 publication ((Bernstein RM, Rassman WR, Szaniawski W, Halperin AJ. Follicular transplantation. Int J Aesthet Rest Surg 1995; 3:119-132.)). This article briefly reviews the salient features of follicular transplantation, discusses how the patient should be evaluated for the follicular transplant procedure, and provides guidelines for the planning of the first and subsequent transplant sessions. This article will address those patients whose balding patterns fall under the major Norwood Classifications ((Norwood OT. Male pattern baldness: classification and incidence. So. Med. J 1975;68:1359-1365.)) as well as those with diffuse androgenetic alopecia. (Please refer to reference 1 for a more detailed description of follicular transplantation and its glossary for the clarification of specific terms. In addition, it is important to be familiar with the Norwood Classification of male pattern baldness, as this will be used frequently in the following text.)
Hair restoration surgery is the single most common cosmetic surgical procedure performed in men in the United States today and is still growing at a substantial rate. Of all cosmetic procedures in men, hair transplant surgery has the potential to produce the most dramatic change in one’s appearance. However, in no other form of cosmetic surgery, has the road to achieving a desired result been more difficult for the patient. Since hair is so visible, the cosmetic problems produced by earlier surgical procedures which resulted in partial, incomplete, or distorted appearances over multiple-staged sessions, often outweighed the long-term benefits.
The protracted course of traditional transplant surgeries that included 2 to 5 mm grafts, scalp reductions, or flaps, used alone or in combination, often produced significant disfigurement. Often, this process represented such an inefficient use of the patient’s time, money, and most importantly his finite donor supply of hair that the work was never actually completed. In the patient who may already have had compromised self-esteem from hair loss, this often had a devastating effect on his overall well-being. In Follicular Transplantation, large numbers of very small follicular implants are used to provide the best possible cosmetic results in the fewest numbers of sessions with the least disruption in the patient’s lifestyle.
Follicular Implants: The Basic Building Block
Follicular Transplantation is based upon the fact that hair emerges from the scalp in naturally occurring groups called follicular units, which are comprised of 1 to 4 terminal hairs. By using follicular units exclusively in the transplant, the surgeon can safely move large quantities of implants in a single session and can create hair patterns that most closely mimic nature. The essence of the follicular approach is that the natural hair groupings of the patient’s hair dictate the size of the implant, rather than the doctor.
The sole use of large numbers of very small grafts for the treatment of androgenic alopecia is not new. First described by Carlos Ubel in Brazil in the early 1980’s, its benefits were more recently popularized by one of us ((Rassman WR, Carson S. Micrografting in extensive quantities; the ideal hair restoration procedure. Dermatol Surg 1995; 21:306-311.)).
Although micrografts represented a significant improvement over the larger grafts, they were not ideal. As the profession gained experience with micrografts, a number of observations were made which suggested that this procedure needed refinement. Micrografts: 1) had a tendency to produce a look that was too thin, 2) often had inconsistent graft growth, and 3) at times required larger sites to accommodate the extraneous skin that was also transplanted.
The advantages of Follicular Transplantation over micrografting are that: 1) a fuller look is achieved, since the grafts are of the same size as seen in nature, 2) growth is more consistent, since the follicular units are left intact, and 3) the results are always natural, since follicular implantation allows the doctor to follow the pattern set by nature in a distribution that mimics the way hair grows in the patient’s own scalp.
Follicular Transplantation enables the surgeon to restore more hair with a minimum amount of transplanted skin. In this procedure, the tissue between the follicular groups is dissected away, while the vital support structures around the units are preserved1. This produces very small “physiologic” implants which, in turn, can be inserted into very small needle sites. By keeping the recipient wounds small, the total surface area of the wound is often significantly less in large sessions of follicular implants than in smaller sessions using larger grafts. Because of the smaller wound size, greater amounts of hair can be safely moved per session. With follicular implants, the accelerated wound healing time and the smaller number of total surgeries required are of great benefit to the patient.
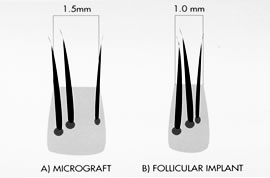 Figure 1. Micrografting vs. Follicular Transplantation. A three hair micrograft (A) that is derived from two separate follicular units may be only 50% wider than a follicular implant (B) derived from a naturally occurring three hair follicular unit, but can have 2 ¼ times the volume of tissue. These differences may be even more dramatic with larger grafts that include multiple follicular units.
Figure 1. Micrografting vs. Follicular Transplantation. A three hair micrograft (A) that is derived from two separate follicular units may be only 50% wider than a follicular implant (B) derived from a naturally occurring three hair follicular unit, but can have 2 ¼ times the volume of tissue. These differences may be even more dramatic with larger grafts that include multiple follicular units.Follicular implants differ from traditional 2-4 mm grafts or minigrafts in that the latter types consist of multiple, partial, or complete follicular units along with the intervening skin. Even micrografts, containing as little as two or three hairs may contain unnecessary tissue if the hair was derived from two or more distinct follicular units (figure 1). Hair moved in non-follicular units (grafts) results in transplanted tissue containing the same ratio of follicles to skin present in the donor area. As healing occurs, the fibrosis that forms around the larger graft contracts bringing the follicular units closer together. This contraction may increase the density of the hair within the graft to the point where it can exceed the density of the donor source. Conversely, if single hair micrografts are derived from splitting up 2 or 3 hair follicular units, the growth may be compromised. In Follicular Transplantation, single hair implants are derived from naturally occurring single hair follicular units so that all the germinative and support structures are left intact.
In all hair restoration surgery, the surgeon is confronted with the problem of having a relatively small amount of donor hair to cover a much larger recipient area (in a patient whose total volume of hair is inexorably dwindling). Therefore, the recipient density should not equal the donor density, much less exceed it. The pluggy appearance of traditional grafts are the inevitable consequence of ignoring this basic principle. If the follicular unit is maintained, the natural hair groups will be held in their normal anatomic relationship, and the appearance will be normal (figure 2).
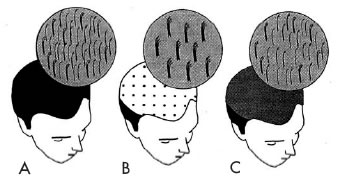 Figure 2. A) Natural hair density. B) Grafts consisting of multiple follicular units. C) Coverage with follicular implants.
Figure 2. A) Natural hair density. B) Grafts consisting of multiple follicular units. C) Coverage with follicular implants.The follicular unit, the basic building block of Follicular Transplantation, consists of 1 to 3, less commonly 4, and occasionally 5 terminal hair follicles. It also includes 1 to 2 vellus hairs, the associated sebaceous glands, subcutaneous fat, and a circumferential band of collagen which defines the unit1. It is essential to have all these elements intact in order to ensure the optimal growth of the implants. The average density of hair in a Caucasian male is 2.0 hairs/mm2 and the average density of follicular units is 1 unit/mm2. Although the density of hair can vary from greater than 3 hairs/mm2 to less than 1 hair/mm2, the density of follicular units is relatively constant.1, ((Headington JT: Transverse microscopic anatomy of the human scalp. Arch Dermatol 1984;120:449-456.)) Figure 3 illustrates the follicular groupings in a non-balding Caucasian male.
 Figure 3. Densitometry showing the natural follicular groupings in a Caucasian male with a density of 2.0 hairs/mm2.
Figure 3. Densitometry showing the natural follicular groupings in a Caucasian male with a density of 2.0 hairs/mm2.The germinative center of the hair follicle is now felt to lie along the region of the follicle, extending from the insertion of the sebaceous glands down to the dermal papillae (rather than just in the matrix) ((Kim JC, Choi, YC. Regrowth of grafted human scalp hair after removal of the bulb. Dermatol Surg 1995; 21:312-313.)), ((Limmer BL. Relating hair growth theory and experimental evidence to practical hair transplantation. Am J Cosmetic Surg 1994;11:305-310.)) but it is clear that the other elements of the follicular unit must also be intact to ensure maximum growth. Whether these supporting structures are directly involved in growth or merely provide protection to the germinative elements during hair transplant surgery has not been resolved, but it is clear that they are necessary to insure follicular survival in the transplant process. ((Seager D. Binocular stereoscopic dissecting microscopes: should we use them? Hair Transplant Forum Int 1996;Vol 6 No 5:2-5.)) The recognition that this naturally occurring biologic unit must be kept “whole” is the fundamental principle of follicular transplantation. Dr. Bobby Limmer has long used, and strongly advocated, stereoscopically assisted microscopic dissection to improve the quality of micrografts. ((Limmer BL. Elliptical donor stereoscopically assisted micrografting as an approach to further refinement in hair transplantation. Dermatol Surg 1994;20:789-793.)) This is equally valuable when follicular implants are used exclusively in the transplant, as it significantly increases the visibility of the follicular anatomy.
Assessing the Extent of Baldness
Anticipating Short and Long-Term Hair Loss
The cardinal rule for the proper planning of every hair transplant is to always anticipate the patient’s worst case scenario. Although any hair loss is never really “predictable,” one must still make an educated judgment as to what the future hair loss will most likely be so that rational short and long-term plans can be formulated.
In anticipating the patient’s long-term hair loss, we find three factors to be useful. Since the inheritance of male pattern baldness appears to be polygenic ((Kuster W, Happle R. The inheritance of common baldness: two B or not two B? J Am Acad Dermatol 1984;11:921-926.)), it is impossible to make accurate judgments from the family history. In our own experience, we find that if a specific pattern of hair loss is recognizable in another family member that matches the patient’s own hair loss pattern and chronology, this can be useful in judging how rapidly the hair loss may progress and what the final pattern might be.
The second factor, the personal history may be of value once the patient has reached his late 20’s. When taking a history, it is important to ascertain not only when the hair loss began, but the present rate of loss. Even for the patient in his late 20’s, it is very hard to predict the future course when the present hair loss is in its early stages. The most difficult of all hair loss patterns to interpret is the Norwood Class III, as this patient has not yet “tipped his hat” as to the direction of future loss.
The third means of evaluating hair loss is to measure the degree of miniaturization in both the donor and recipient areas. Miniaturization is the progressive diminution of hair shaft size reflected in both the diameter and length, due to the genetically determined effects of aging and/or androgenic hormones on the terminal hair follicle. We find that miniaturized hairs normally represent no more than 20% of the terminal hair population. Because miniaturization is a relative measurement (comparing finer hair to the thickest hair), it takes substantial experience before this measurement can be useful to the individual clinician. In our experience, from examining and following, over 5,000 patients with the Hair Densitometer ((Rassman WR, Pomerantz, MA. The art and science of minigrafting. Int J Aesthet Rest Surg 1993;1:27-36.)), we have found that assessing the degree of miniaturization has useful predictive value when evaluating the risks of hair loss and in establishing hair loss patterns. A high degree of miniaturization in the upper portion of the donor area suggests that the donor fringe will contract over time. A high degree of miniaturization throughout the donor area indicates that all of the patient’s hair is unstable and that he is at risk to have diffuse unpatterned alopecia and of becoming extensively bald (see section on Diffuse Androgenetic Alopecia).
Miniaturization in the recipient area can often delineate which areas of the scalp are most likely to bald and which are stable, anticipating the patient’s future Norwood classification. In the very early stages of hair loss, increased miniaturization can anticipate future balding even before any loss is clinically apparent. Usually large numbers of hairs undergo miniaturization before any are actually lost. Therefore, even with clinically significantly thinning, the actual total number of hairs present in the balding area may be the same as the patient’s original hair counts. The percentage of terminal hairs, however, would be markedly diminished. For the most reliable prediction of the final hair loss pattern, the patient should be over the age of 30 and have had significant hair loss already, although this measurement is, of course, useful at any age.
As mentioned above, predicting future hair loss in the Class III patient is especially problematic. In contrast to the Class III Vertex patient, who we may reasonably expect will evolve into a Class V or VI (especially if there are Class V or VI family members), it is impossible to accurately predict if the Class III patient will stabilize and remain at this class or will become more extensively bald. However, a significant degree of miniaturization (>20%) measured in a young person across the top and crown, but sparing the bridge, would suggest the likely possibility of future progression to at least a Class IV or V (and possibly to a Norwood Class VI or VII pattern). Widespread areas of increased miniaturization throughout the front and top of the scalp indicate the development of either diffuse, patterned or unpatterned alopecia (see section on Diffuse Androgenetic Alopecia).
We feel that in predicting the short-term loss, the extent of miniaturization in the recipient area, as well as the rapidity of the loss, are important. In rapid hair loss, the degree of miniaturization in the balding area is well over 50%, and this can be easily determined with the densitometer. Often the reason a person seeks a consultation for hair loss is that there is some change in the “rate” of his hair loss. A patient who is gradually losing his hair is less likely to seek help than a patient who suddenly has an acceleration in the rate that he is losing hair. However, it is the very patient who is first seen while entering an accelerated stage of hair loss that is at greatest risk for being unhappy with the outcome of his surgery. Careful counseling to give him a clear understanding of the natural progression of his balding is critical in achieving realistic patient expectations. In treating patients with rapid hair loss (and adequate donor reserves), goals must be conservative and clearly defined before hair restoration surgery is attempted.
A history of diffuse, rapid hair loss, especially in a young patient, can be an ominous sign and may reflect an evolving Norwood VII pattern. This is often associated with a high degree of donor miniaturization, significant bitemporal recession, and the absence of the elevated triangular segment of hair in the parietal region that would define a Norwood Class VI. (The superior portion of the rim of Class VII patient, when viewed from the side, is flat, or slopes gently backwards. This is in contrast to the Class VI patient who, when viewed from the side, has an elevation, that has its peak just anterior to the ear and is the residual of the Class V bridge that separated the anterior and posterior portions of the scalp.) Occasionally, a young patient is seen with a complaint of loss of hair volume, but that clinically appears to be normal. If densitometry reveals a donor density in the range of 1.0 to 1.5 hairs/mm2, with miniaturization in this area of 35% or greater, this patient has a high risk of being extensively bald with insufficient donor hair and, in our opinion, should generally not be transplanted.
Planning for an Effluvium and Progressive Hair Loss
Hair transplantation often produces varying degrees of effluvium (shedding) in the recipient area. The hair in the implants generally undergo an “anagen” effluvium which results in shedding that begins within two weeks post-op and generally involves over 90% of the transplanted hair population. In contrast, the patient’s original hair in the recipient area (in the vicinity of the implants) may be shed in a “telogen” effluvium. Telogen effluvium usually occurs after a 2-3 month delay, and the loss rarely exceeds 50% of the hair population. The diagnosis can be made by examining the hairs. Hairs in anagen effluvium are terminal hairs that show specific dysplastic changes. Hairs lost in telogen effluvium are morphologically normal resting hairs ((Demis DJ. “Clinical Dermatology.” Philadelphia, PA: J.B. Lippincott Co. 1994, (1) 2-35 p3.)).
The hair that is subject to being impacted by a telogen effluvium is usually miniaturized hair. Healthy terminal hair or hair from previous transplantation procedures, are much less likely to be affected. Each miniaturized hair is of smaller diameter and shorter length than the corresponding terminal hair and may not have great importance individually, but since these hairs often can be present in large numbers, they can have a substantial clinical impact. In later stages of hair loss, the balding area may be populated entirely by miniaturized hair.
Telogen effluvium is generally more significant during active stages of hair loss. This hair loss can be substantial in the young patient who is rapidly balding and whose recipient area is characterized by a high degree of miniaturization. When the effects of telogen effluvium are superimposed upon hair that is already near the end of its natural life span, this shed hair often does not return. Unless a significant amount of hair is transplanted in these individuals, the gain from hair transplant surgery may not be adequate to compensate for the loss due to the telogen effluvium. It is important to explain to the patient that when performing a transplant in the early stages of balding, large numbers of miniaturized hairs will be replaced by a relatively smaller number of healthy terminal hairs. Although the density can never reach that which was originally present, the overall clinical appearance may be improved, because these terminal hairs will have the size and luster of his original hair, and may produce a fuller cosmetic appearance. The major gains, however, will be to provide a permanent frame for the face and avoiding the problem of having to wait to become more bald in order to have a procedure. In the surgical planning, when a significant amount of miniaturization is present, the numbers of implants used should approach that which would have been planned if the area was totally devoid of hair.
It is important to note that it may not only be the actual trauma of making the sites that induces this effluvium, but the vasoconstrictive properties of the epinephrine and other factors may be contributory. In this regard, transplanting a small number of grafts may not offer any great protective advantage over transplanting large numbers. On the contrary, we feel that it is probably important to transplant enough hair to overwhelm any possible telogen effluvium that might occur so that the net effect of the transplant will be a positive one.
We find donor density and scalp laxity to be the key factors in determining the total donor reserves of the patient. The number of follicular units in the mid-portion of the donor area of a non-surgically treated, normal Caucasian male is 1 unit/mm2 (see ref. 4). Thus, in the first procedure, the donor area should yield one follicular implant per mm2 of scalp harvested if there is no wastage during the surgery. However, there will always be a fraction of the grafts lost from harvesting the strip and some loss from dissection of the individual units, depending upon the skill of the surgical team, which must be accounted for. In longer strips, as both the back and sides are accessed, the density will often decrease toward the temples. This must also be taken into account. In some individuals, the density can vary widely within a localized area. There will also be errors due to the visual limitations in identifying the hair, particularly in those patients with white hair. Telogen follicles, which represent about 10% of the total population, will not be visible with densitometry or under gross visualization (if the hair has been shed), but can be seen with the aid of the dissecting microscope.7
Since the number of follicular units per unit area is constant, the donor density will tell us the average number of hairs per implant (i.e. it will tell us the quality of each implant). Thus, if a patient has a density of 2 hairs/mm2, the donor area will contain one follicular unit per mm2, and the implants will consist of an even mix of 1’s, 2’s, and 3’s, with the average being 2 hairs per implant. If a patient has a density of 2.3 hairs per/mm, there will still be one follicular unit /mm2, so the same number of implants will be harvested per unit donor area, but now the implants will have an average of 2.3 hairs/mm2 and consist of a mix of 1’s, a larger percentage of 2’s and 3’s, and even some 4 hair units.
If the scalp has been stretched from previous hair transplants, scalp reductions, or scalp lifts, the follicular units will be spaced further apart, and it will be necessary to actually measure the density of follicular units to accurately estimate the number of implants obtainable from the strip (as the density of follicular units will now be less than 1/mm2).
Donor scarring from previous surgeries will also have a significant impact on the ultimate donor yield. There will always be some loss of hair as a result of the actual scar produced by any donor harvest, no matter how perfectly executed. In addition, the angle of the surrounding hair in the immediate vicinity of the scar will be altered slightly so that there will be more transection in any subsequent harvest. This effect has been reduced, since the use of the multibladed knife has been abandoned by these authors and replaced by two parallel blades, with adjustable spacing, angled at 30o. In addition, the use of tumescence in the subcutaneous fat, increases the margin of safety below the follicles when harvesting the implants. However, even with these improved techniques, the blades still may damage more hair follicles in scarred rather than virgin scalps, due to the altered angle of the remaining hair. Racial differences will also have a significant effect upon the number of implants that may be harvested per unit area.
A person can lose a substantial amount of his/her hair volume before any change is noticeable. When the hair is blonde or white, more hair can be lost before the thinning is evident. When the hair is black and the skin white, thinning may be evident even sooner. This loss in volume can either be due to actual loss of hair or due to the decreased volume of each individual shaft from miniaturization. In our experience, in a person with average density and average hair attributes, half of the donor area may be moved without a significant change in appearance. However, in a person whose normal donor density is 25% below average, (i.e. 1.5 hairs/mm2 rather than 2.0 hairs/mm2) there would be a 50% decrease in moveable hair since the same fixed amount (1.0 hairs/mm2) must still remain for the donor area to look natural (for more details see ref. 1, table 1). As discussed above, the assessment of miniaturization (the progressive diminution of hair shaft size) must always be part of the evaluation. A high degree of miniaturization in the donor area can mean that a significant portion of the patient’s donor hair is unstable, and this must be accounted for in the long-term surgical planning.
While donor density was thought to be the critical factor in determining the patient’s ultimate donor supply, it appears that scalp laxity plays a much greater role in the total availability of donor hair than had been previously imagined. In a patient with a loose scalp, the harvesting of the donor strip merely removes some of the scalp redundancy and has little impact on the density. With a tight scalp, however, each procedure stretches the skin, producing a measurable decrease in the density (hairs/mm2). The full impact of a tight scalp is not usually appreciated at the first surgery, but on subsequent procedures the ability to produce a non-tension closure and to harvest a significant amount of hair (in the face of decreased density) can be severely compromised. In a patient with a scalp that is tighter than normal, the long-term goals must be scaled back to coincide with a more limited donor supply. The adverse effects on scalp laxity, as well as donor density, are among the many reasons why scalp reductions are not recommended by these authors ((Bernstein RM. Are scalp reductions still indicated? Hair Transplant Forum Int 1996; Vol 6(3):12-13.)).
The dimensions of the donor area are also very important. We measure the length of the donor region from 3 cm behind the temple hairline to the corresponding part on the other side. This distance should be at least 30 cm. If it is less, more conservative goals should be considered. As mentioned previously, recession at the temples can be a sign of extensive balding, and densitometry should be performed to assess the stability of the temple hairline position. The height of the permanent zone is equally important and this distance can vary markedly, even from one Norwood Class VII patient to another. Again, densitometry can measure the extent of miniaturization which is useful in assessing what the future dimensions of this region might be.
What Can Be Accomplished in The First Session?
Patient Expectations
In our experience, patient expectations are most often influenced by the patient’s age, stage of hair loss, and its rapidity. The young patient (those in their 20’s) with the memory of their adolescent hairline and density still clear in their minds, are also the ones most susceptible to rapid, significant hair loss and are the patients that need the most time in the education and planning process. Other factors include the person’s social situation (such as how he is perceived by significant others), and how he has been dealing with his hair loss (such as using a hair piece or the continuous wearing of a hat). It is incumbent upon the physician to educate the patient and set his expectations correctly, or the patient may never be satisfied.
The patient should not be led to believe that hair restoration surgery will restore what has been lost. In the ideal situation, hair restoration surgery should maintain the patient’s adult appearance and give him the same “look” as he would have had if he had simply “matured.” The surgery should never attempt to restore the patient’s adolescent appearance. At a minimum, it can keep the patient from perceiving himself as being bald. In a patient who is distraught from extensive hair loss, this alone can be a significant accomplishment.
The young, rapidly balding patient poses perhaps the greatest challenge. Even an extensive procedure may not be able to compensate for the loss that can occur during the year it takes for the implants to fully grow. In this patient especially, understanding every aspect of the dynamic nature of the hair loss is critical. The progressive nature of balding, realistic hairline placement, the sparing of the crown, and the possible acceleration of loss from the surgery itself must be clearly explained. If the patient does not grasp each and every one of these ideas, it is better to postpone the surgery. Time is always on the physician’s side, since the progression of the patient’s hair loss will make each of these issues more tangible to the patient, simplifying the education process.
At the other end of the spectrum, the patient who has been bald for many years is much easier to satisfy since his expectations are generally reasonable, and modest amounts of hair will produce a marked change in his appearance. However, this same patient who has worn a hair piece for many years identifies with this look and is much more difficult to please. Like the very young patient, his reference point is a full head of hair. If this patient’s only goal is to be rid of the hair system, it is critical to determine the necessary amount of coverage that would be needed to accomplish this. If this has not been established beforehand, a transplant that might be perfect in every other respect, will be a total failure if the patient still feels compelled to wear his hair piece.
Different problems are presented by patients with more limited hair loss. The person who presents with recent progression from an adolescent hairline (Norwood Class I) to a mature hairline with natural recession at the temples (Class II), should not be transplanted. It should be explained that this evolution is normal and a flat hairline would look unnatural as he ages. In this patient, one should not attempt to “fill-in” the temples. It also may not be appropriate to transplant a young, early Class III patient. However, in an older Class III patient with stable hair loss, above average density, and without a familial history of significant balding, it would be appropriate to blunt the angles produced by the bitemporal recession, but not to eliminate it.
A final issue regarding expectations is related to the time frame in which the patient expects to see the results of his procedure. The normal follicular growth cycle is quite variable. In most patients, the majority of the transplanted hair begins to grow at about 3 to 4 months after surgery, with additional hair appearing over the next several months. In a small percentage of patients, the onset of growth of the bulk of the hair can be seen from 4 to 8 months or more, with additional new hair occasionally appearing up to 18 months after the transplant. Since newly transplanted hair will increase in diameter and in length, in this subset of patients, there may be continued cosmetic improvement for up to two years.
There has been much speculation regarding this so called “delayed growth,” and it appears that a number of factors may be contributory ((Bernstein RM, Rassman WR. What is delayed growth? Hair Transplant Forum Int 1997; 7 no.2.)). Although still speculative, some of these include: 1) the normal asynchronous nature of human follicular growth cycles, 2) the possible resetting of the growth cycle after the post surgical effluvium (shedding) to a new full cycle, 3) the staggering of hair regrowth after the post surgical shedding, 4) retarded growth as a result of graft trauma such as temperature change, desiccation and crush injury, 5) amputation of the dermal papillae during graft dissection with a time lag for it to regenerate from the bulb, ((Cooley J, Vogel J. Loss of the dermal papilla during graft dissection and placement: another cause of x-factor? Hair Transplant Forum Int 1997; 7:20-21.)) and 6) local factors causing delayed growth, such as the often asymmetric elastotic changes in the skin caused by the sun reaching the unevenly protected balding scalp.
Carefully controlled studies, some of which are already in progress, will be needed to sort out the relative importance of each of these factors. Regardless of the cause, it seems that great individual variability is an integral part of the transplantation process. This must be clearly explained in advance in order to keep our patients from becoming “impatient” after hair transplant surgery.
The Critical Session
Regardless of how many procedures are planned, we feel that one should always regard the first transplant as the critical procedure. The patient views the first session as a statement of future sessions. The first session builds confidence, so it is essential that expectations are met. The first session is the most important, for it is the one that generally establishes the hairline and frames the face. The initial transplant also places hair in a position to camouflage subsequent procedures.
In our experience, for the majority of patients, establishing the frontal hairline is the single most important function of the first procedure. At the outset, the frontal hairline should be placed in its normal, mature position. The hairline in this location should frame the face and restore a balance to the patient’s facial proportions in a way that is appropriate for a mature individual. In our opinion, the common practice of creating a hairline significantly above the mature hairline position with the intention of lowering it in a subsequent procedure should be avoided. If the intent is to conserve hair in anticipation of a very limited donor supply, one could still maximize the cosmetic impact of the surgery by creating more bitemporal recession or not extending the transplant as far back toward the crown. However, the position of the mid-portion of the frontal hairline should not be compromised, as this defines the “look” of the individual. Creating a hairline too high (in the hope of conserving donor hair) only accentuates the patient’s baldness by enlarging the forehead and distorting the normal facial proportions.
The other major goal of the first session should be to provide coverage to the remaining bald scalp with the exception of the crown. Since the Norwood Class A patients, by definition, do not have hair loss extending into the crown, if possible, their entire bald area should be treated in the first session. The amount of hair needed to cover the front and top of the patient’s scalp will obviously vary depending upon the extent of baldness, but there should always be an attempt to cover these areas in the first session, even if the coverage is light. In general, areas of the scalp which already have adequate coverage should not be transplanted. Although the edges of the transplanted area should be blended into the hair bearing skin, too aggressive encroachment may accelerate hair loss and not offer any additional cosmetic benefit. The goal should not be to restore adolescent density, since this is neither necessary from a cosmetic standpoint nor (as we have discussed) mathematically reasonable. Patients desiring adolescent density should be treated the same as those desiring an adolescent hairline. They should be further educated rather than ushered off to surgery.
In general, crown coverage should not be a goal of the first session, but should be addressed after the cosmetically more important front and top have been adequately transplanted. Since the front and top of the scalp are a single cosmetic unit, the transplant may stop after this area has been treated. The patient can then evaluate for himself the adequacy of coverage from the first procedure, and if he desires more fullness or greater density, a second session can be used to supplement the area transplanted in the first. If crown coverage is attempted in the first session, the patient’s options will be much more limited, and the ability to produce an aesthetically balanced transplant might be permanently eliminated. An exception would be patients of Norwood Class III Vertex and Class IV, who are generally over the age of 30, have less risk of becoming extensively bald, and have good donor density and scalp laxity. In these situations, transplanting the crown in the first session can provide modest coverage to the area and will serve to camouflage a limited amount of further crown balding. What should be avoided in these patients is the risky practice of repeatedly transplanting hair into the crown to achieve a high degree of density, as this density can often not be supported as the balding progresses (see section Goals for the Second Section).
Beside the aesthetic issues which make the first session so important, there are many surgical advantages of working on a virgin scalp1. In sum, implants can be placed more easily, more securely, and closer together into a normal scalp, since the blood supply and elasticity of the connective tissue are intact. In the donor area, maximum density and scalp mobility as well as the absence of scarring will facilitate a hairline closure. To take advantage of these factors, one should attempt to achieve, in the first session, as many of the patient’s goals as possible. In our opinion, what can safely be accomplished in one procedure is best done in one procedure, and should not be spread out over two or more.
When Should a Single Session Transplant be Considered?
A great deal can be accomplished in the first session. However, one must be realistic in anticipating what goals may be achieved with a single surgical procedure and in which patients these goals are possible.
As stated, we feel the main goals for the first session should be: 1) to provide a frame for the face, 2) to provide coverage to the front, and, when appropriate, the top and vertex of the scalp, 3) to have a totally natural appearance.
In general, for the physician to suggest to a patient that he might be satisfied with a single session, he should have relatively stable hair loss. This is especially important in the Norwood Class III, IIIa, IV, and V patients whose own hair contributes to the cosmetic appearance of the front of the scalp. In patients who have little frontal hair, the first procedure may successfully frame the face and provide coverage to the anterior portion of the scalp so that even with further balding, a second procedure would not be immediately necessary. For Norwood Class VI or VII patients in which the front and top of the scalp are adequately transplanted in the first procedure, satisfaction can be achieved in one session, because further expansion of the bald crown is relatively inconsequential. However, if coverage of the crown was attempted, then as the bald crown expands, the centrally transplanted grafts would become an isolated island of hair, and further surgery would be required.
A patient with lighter hair color will also have a greater chance of achieving his goals in one session as these colors reflect light and give the appearance of more hair. In addition, the low contrast with the underlying skin gives the illusion of more hair since the skin serves as a “filler” for the space between the hair shafts. In contrast, dark hair over light skin accentuates any spaces between the strands of hair. Salt and pepper hair works both by reflecting light and by creating another visual detail to detract from areas of sparseness. Certainly any patient who does not posses the genetic attributes of good hair color can easily change the color to complement the surgical procedure.
Wavy hair will generally provide better coverage than straight hair and is beneficial in the transplant. As with hair color, this can be manipulated after the surgery to improve the cosmetic impact of the transplant. Very curly hair, on the other hand can, on occasion, work to the patient’s disadvantage if complete coverage of the bald area is not anticipated. Very curly hair may increase the fullness of the transplanted area to such a degree that contrast with any remaining bald area may be accentuated. In addition, very curly hair transplanted to the front and top of the scalp may not be easily combed back to cover a bald crown.
The follicular density in the donor area will also impact the procedure. In patients with high density, there will be more hairs per follicular unit, and thus each implant will contain more hair. In patients with very high density, a significant proportion of implants containing 3 and 4 hairs each can be harvested from the donor area, giving a wonderfully full appearance, even from a single procedure.
Patients with hair of average or above-average diameter will have the best chance of success with one procedure. The cylinder of skin surrounding the follicular unit of a patient with coarse hair is roughly similar to a unit of fine hair, however, the volume of hair is vastly different. The diameter or “weight” of the patient’s hair is a huge variable. Whereas density may vary by a factor of 3 fold, hair weight may vary from patient to patient by many times that. Although it is much easier to quantify the density (number of hairs/mm2), rather than the weight of an individual hair, the latter is probably more significant to the outcome of the procedure. Those patients with early balding who have fine, dark hair of high density are very difficult to satisfy in a single session, since the transplanted hair is often viewed against the background of the patient’s thick terminal hair population that surrounds the bald area. By contrast, in a similar patient with coarser hair, satisfaction is more easily achieved in a single session.
Contrary to what one might expect, the extensively bald patient, even with low donor density, can often be very satisfied after one procedure. These patients often have very reasonable expectations and after being bald for many years are ecstatic to have hair framing their face, light coverage on top, and “something to comb.” In order for expectations to be met in one session, the realities of the supply/demand situation must be taken into account. It is obvious that for individuals in the Norwood Class VI or VII pattern, only light to modest coverage can be achieved in a single session, since the area in need of hair will exceed the total donor supply by a factor of at least 6:1, even under ideal circumstances.
Finally, grooming patterns will also influence the success of a single procedure. Patients who plan to comb their hair to the side rather than straight back will have the appearance of much more fullness. Unfortunately, this hair style will not provide crown coverage. Many patients achieve the “best of both worlds” by combing their hair diagonally backwards.
Planning a Second Hair Restoration Session
When Will a Second Session be Needed?
It is important for the patient’s social and financial planning to honestly discuss, at the outset, the likelihood, the frequency, and the cost of subsequent transplant sessions. As discussed above, a second session will usually be needed in patients with less than optimal hair characteristics. In addition, a second procedure may be required in very bald patients with low donor density and/or reduced scalp laxity, as these factors limit the amount of hair that can be harvested at any one time. In these situations, anticipating a second hair transplant surgery in the near future is a critical part of the initial planning, unless the patient is willing to accept a thinner look. A second procedure should always be anticipated from the outset in younger patients who are early in the balding process, when hair loss is rapid, and in patients of Norwood Classes III through V, whose balding does not appear to be stable (see section Predicting Short and Long-Term Hair Loss).
A special situation exists when transplanting patients with a persistent frontal forelock. The density of a forelock is often close to the patient’s original frontal density, making it impractical to place additional hair into this area. Although the forelock tends to be very tenacious in some families, it still may show a slow rate of loss. If lost, a gap would be left in the central portion of the frontal hairline, making a second procedure necessary as soon as this should occur.
Timing of the Second Session
Hair growth after transplantation is quite variable. On the average, growth usually starts in about 3-4 months with the hairs gradually increasing in both thickness and in length so that the first half inch is often not reflective of the long-term quality and weight of the hair. In a small number of individuals, probably 2-5%, the implants begin to grow almost immediately. As discussed in the section Patient Expectations, growth may occasionally be delayed for up to a year or longer. Hair growth generally occurs in waves, with a few weeks (sometimes months) between growth spurts. There may also be some variability from one region of the scalp to another.
If the goal is merely to add more hair and increase fullness, this can be done at any time after the transplanted hair can be identified. However, for the full cosmetic impact of the procedure to be appreciated, one must generally wait at least 8 to 12 months. During this time, the continued increase in the diameter and length of the hair will significantly alter the final appearance. Once the hair is at styling length, both the patient and physician can make aesthetic judgments regarding the weighting and balance of additional implants. Therefore, decisions about future hair transplant surgery should be deferred until that time.
It will also be advantageous to delay the next procedure to maximize the donor harvest. Although each hair restoration procedure results in a potentially tighter scalp, some of the pre-operative donor laxity returns in the months following the surgery. The major change will occur during the first month as the edema and inflammation subside. Further loosening will occur as the scalp stretches over the next 6-12 months. The amount of laxity can be maximized by keeping the donor excision very superficial. If the dissection is limited to the mid-fat, then the dermis will continue to move freely over the fascia below. Once the fascial layer is penetrated, healing may obliterate the subcutaneous layer and significantly decrease scalp mobility.
In the uncommon event that there is a telogen effluvium in the donor area, the telogen follicles may not be easily identifiable in the dissection. Since recovery in the donor area may take up to a year, it is essential that one wait until complete regrowth occurs before a second session is attempted. Rarely, if the closure was too tight, the effluvium may eventuate in permanent hair loss, and this would present a distinct cosmetic problem that should be addressed before any additional hair can be harvested.
As a general rule, to allow for optimal healing and hair growth in both the donor and recipient areas, we encourage the patient to wait at least 8 – l2 months before considering a second procedure, unless the surgeon is going to transplant an area of the scalp previously untouched.
Goals for the Second Session
We find that the most common reason a second session is performed is to enhance the appearance of fullness. Although follicular units may have been placed as close as possible in the first session, after healing has occurred, additional units can always be added between the first implants. Any decision to increase the density of any given area must, of course, be made in the context of anticipating any possible future hair loss and the limitations of the donor supply. Expending donor hair without fully appreciating these two factors will always negatively impact the patient’s long-term result.
Another reason for a second session is to follow the progression of the hair loss. This is often performed in conjunction with increasing the fullness of the previously transplanted areas. Usually at the second session, more density is added to the cosmetically critical front and top of the scalp, and then the transplant is extended further back either to compensate for any additional hair loss that may have occurred since the last procedure. A second procedure may also be used transplant an entirely new area, such as the crown, knowing the front and top are secure.
A third “goal” of the second session is to further refine the hairline. Since in the initial planning of the first session, placing the frontal hairline in the most appropriate position was a priority, major changes in the hairline should not be necessary. However, subtle adjustments in the hairline are usually needed both because of the limitations of a single session, and because it is impossible to anticipate exactly what the cosmetic impact of any procedure will be. Some of the refinements include: 1) making the frontal hairline more dense, 2) increasing the irregularity of the transition zone, 3) flattening the hairline or slightly blunting the corners, 4) lowering the hairline, 5) establishing a widow’s peak, and, in very select cases, 6) restoring the temples.
We feel that the primary decision of the second session should be whether or not to transplant the crown. This decision is important, because once treatment of the area has begun, it can potentially place huge demands upon the donor supply. Many insightful patients who are significantly bald realize that crown coverage is not realistic and are satisfied using styling techniques in conjunction with creatively distributed transplants to maximize coverage in the lightly or non-transplanted areas. This is especially true in older patients. On the other hand, a substantial number of people are very bothered by their bald crown and have this as their main focus. It is, however, the very patient who is bothered by early crown balding that may be devastated when hair loss occurs in the front. For most patients, crown balding becomes much less important when it is compared to the prospect of losing frontal hair and the frame that it provides to the face. Crown balding will also become more acceptable as the patient ages (as will his hair loss overall). It is, therefore, incumbent upon the physician to assist the patient in setting priorities that will be appropriate over the long-term.
If not treated in the first session, the crowns of Norwood Class III Vertex and Class IV patients may be transplanted in the second session with the same considerations of age and donor supply as in the first session (i.e. over the age of 30, have little risk of becoming extensively bald, and have good donor density and/or scalp laxity). In the second session, we generally consider treating the crown in older Class V patients if they have stable hair loss and average or better-than-average donor density (> 2 hairs/mm2) and/or good scalp laxity. Patients of Norwood Class VI can be treated similarly, but they should have more conservative goals. Occasionally, a Class VII patient with high density and a very lax scalp can have their crown transplanted. The Class Va patient can be treated with more impunity in the second session, especially if the front and top have had good coverage from the first session, and if the Class Va patient has pure “Vertex” balding, rather than extension into the crown.
If extensive balding is a likely possibility and the patient has only a modest donor supply, it is always best to treat the crown as an extension of the top, rather than as an isolated region, to ensure that he will not be short of hair, if the intervening region were to bald. This is the reason we feel that the treatment of the crown in the “average” Class III Vertex and Class IV patient should be delayed. At times, the Class V patient has lost enough hair in the “bridge” that the surgeon can transplant “through” this area in the first session. By the second session, the surgeon is able to assess if there is enough coverage of the front and top to attempt the crown. It is important to emphasize that when crown coverage is considered in the second session, the transplanted hair in the front and top has already been allowed to grow, so that its cosmetic impact can be assessed. The patient can thus make his own aesthetic judgments regarding whether or not to add additional hair to this area before transplantation of the crown is begun.
The issue of crown coverage is so important, because it is the least visible of the balding regions, but can potentially occupy a very large surface area, producing an almost inexhaustible demand upon the donor supply. The predominantly anterior-posterior progression of frontal balding allows the transplanted hair to conceal hair loss behind it. It is common to see a person with frontal hair and a bald area in back (or less commonly isolated from the sides). Therefore, as balding continues after a transplant in the frontal area, a natural look is maintained. In contrast, the crown expands centrifugally, so that as crown balding progresses, the initially transplanted hair may become a cosmetic liability rather than an asset. This is because with further hair loss, transplantation must be continued, or there will be an isolated island of hair surrounded by a moat of bald skin. In addition, the density of the normal crown increases as one moves away from the center. Thus, whatever is transplanted outward must have at least the density of the part more central to it. Whereas the initial transplant of frontal hair can be followed on subsequent sessions by placing less density behind it (or not treated again), with crown balding, the reverse is true. The expanding crown will always require a subsequent session of at least the same or increasing density in an area that is ever increasing in size. This discussion seems very logical, but too often a surgeon will treat early crown balding by trying to match the surrounding density with larger grafts or multiple sessions of smaller grafts, only to leave the patient with a density that can never be sustained as the balding progresses.
An important alternative to the treatment of the crown is to stop the transplant at the vertex, and have the patient groom his hair back over the non-transplanted area. This is recommended for patients when direct crown coverage is not realistic, or when it is too early in the balding process to determine whether or not significant crown coverage will be possible in the future. Another advantage of sparing, or lightly covering the crown, is that donor reserves may be saved to address further diminution of the donor fringe.
Subsequent Hair Transplant Sessions
For the reasons discussed, we feel that one should attempt to accomplish the patient’s goals in one or two sessions, although, of course, this is not always possible. Obviously, it is not possible in actively balding patients, and it is for this reason that a transplant in these patients should often be postponed. For the Norwood Class III, IV, and V patients that appear to be stable, it is important for the physician to give a realistic assessment of the time frame in which he expects the balding to continue so that the patients can make reasonable decisions regarding their present and future surgeries. This, of course, must be done with the understanding that time frames may not always be predictable, and that hair loss is generally inexorable. In the Class VI and VII patients, even with further hair loss, additional surgery may not be needed if the initial procedures were planned properly.
The important point is not that the patient be guaranteed that all his hair loss problems will be solved in one, two, or any number of sessions but that the surgeon should make every attempt to accomplish the restoration in as few sessions as possible, rather than to engage the patient in an unnecessarily protracted course of multiple surgeries.
The number of implants required to achieve patient satisfaction varies widely due to the great variability in individual hair characteristics. In addition, since hair loss patterns are a continuum, and the Norwood classes discrete, the number of implants needed for each class can vary significantly. The number of follicular implants that we generally transplant in the first session has been summarized in a previous publication (ref. 1, table 3). We feel that the following approximate total number of follicular implants are needed for a complete restoration without and with crown coverage (table 1).
Table 1. Total Number of Follicular Implants Suggested for a Complete Restoration.
A satisfactory restoration does not necessarily imply that complete coverage of the entire bald area necessarily be achieved. The finite donor supply often limits what can be accomplished, regardless of the hopes of the patient or the abilities of the surgeon. The specific attributes of the patient’s hair and the nature of the patient’s expectations will, of course, affect how satisfactory the final results will be. With an aesthetically planned transplant, many patients can achieve satisfaction with a lesser number of grafts than the above table would suggest. For those patients with less than optimal hair characteristics or those with higher expectations, the numbers may be greater.
When needed, the planning of subsequent procedures follows the general concepts discussed in the section Planning a Second Session. It is most important to remember, however, that regardless of the patient’s insistence that a certain level of fullness or density be achieved, all judgments must be made in the context of the patient’s finite donor supply.
Managing the Patient with Diffuse Androgenetic Alopecia
Definition and Types
In addition to the regular Norwood Classes (I to VII) and the Norwood Class A’s (Ia to Va), there are two other types of male baldness that O’tar Norwood has termed “Diffuse Patterned Alopecia” and “Diffuse Unpatterned Alopecia.”2 Although these patterns receive little attention, they appear to be quite common and present special problems for the transplant surgeon. We have attempted to further define and stage these two types of balding in order to gain insight into their appropriate management.
Diffuse Patterned Alopecia (DPA) is an androgenetic alopecia characterized by diffuse thinning in the front, top, and vertex of the scalp in conjunction with a stable permanent zone. Diffuse Patterned Alopecia is usually associated with the persistence of the frontal hairline represented by the hairline position of the Norwood Class II or Class III patient. Especially in the earlier stages, the thinning generally extends to the vertex without significant hair loss in the crown. It differs from the regular Norwood classification in that, when the hair loss is first noted, it is already in a stage resembling a thinning Norwood Class VI, rather than having progressed through the Norwood stages III, III Vertex, IV, and V, which are characterized by continued recession at the temples, an expanding vertex/crown, and the presence of a defined bridge separating the anterior and posterior portions of the scalp. In addition, there is an absence of the residual triangular elevation in the parietal region that helps to define the typical Norwood Class VI patient.
Diffuse Patterned Alopecia differs from the less common Diffuse Unpatterned Alopecia (DUPA) which is also androgenetic, but lacks a stable permanent zone. Diffuse Unpatterned Alopecia patients have a similar progression of balding as the DPA patient except that the progression is often more rapid and will more likely eventuate in a “horseshoe pattern” resembling the Norwood class VII, except that in contrast to the Norwood VII, the DUPA “horseshoe” can look almost “transparent” due to the low density. The differentiation between DPA and DUPA is critically important because DPA patients are often good candidates for an appropriately timed transplant, whereas DUPA patients should almost never be transplanted because they will inevitably have extensive hair loss without a stable zone in which to harvest the hair.
Both Diffuse Patterned and Unpatterned alopecia also occur in women. However, in contrast to men, the DUPA in women is much more common, probably occurring 10 times as frequently as DPA. As in men, the female DUPA patients are not good candidates for a transplant (except in the instance where the donor hair is used solely to soften the frontal edge of a wig). The high incidence of Diffuse Unpatterned Alopecia in women partly explains why so few women have their hair transplanted. It is also important to emphasize that a non-androgenetic differential must be considered in all unpatterned alopecias. This is especially true in women, where a host of medical conditions can produce diffuse unpatterned hair loss including anemia, thyroid disease, connective tissue disease, gynecological conditions, and severe emotional problems.
We find densitometry to be helpful in distinguishing Diffuse Patterned Alopecia from Diffuse Unpatterned Alopecia. A donor density in the range of 1.0 to 1.5 hairs/mm2 with donor miniaturization in excess of 35% indicates an unstable permanent zone and precludes a diagnosis of DPA. As discussed in the section “Predicting Short- and Long-Term Hair-Loss,” these densitometry readings in a younger patient, even with little clinically apparent hair loss, point toward a high risk of extensive balding. The importance of densitometry is that not only will it help to distinguish between DPA and DUPA, but it can help to predict which patient will not be a good candidate for a transplant even before visible balding has begun.
Staging
The diffuse androgenetic alopecias, that we will refer to simply as DA and which consist of Diffuse Patterned Alopecia (DPA) and Diffuse Unpatterned Alopecia (DUPA), can be further divided into various stages of progression with DA0 representing the pre-balding state. The earliest stage of loss, in these diffuse alopecias, DA1 , would be characterized clinically by a “slightly thinning” look in the front, top, and vertex, best visualized under strong lights or when the hair is wet. At other times it might not be noticeable. Almost all patients have subjective complaints of less fullness in the affected areas. Preliminary densitometry studies in the thinning area of these patients have revealed miniaturization to be in the range of 20-50%. DA2 represents the stage when there is obvious thinning evident under normal lighting, but if the hair is styled properly, the degree of hair loss may be acceptable. Miniaturization for DA2 is on the order of 50-75%. Patients with DA3 have significant hair loss in the transplanted area, and the coverage it provides is no longer adequate. The frontal hairline, though still recognizable in it’s position as the mature hairline, does not have enough density to frame the face. Miniaturization in DA3 is usually around 75-95%. The DA4 patient has lost most of his terminal hair in the balding area (miniaturization > 95%), generally has involvement of the crown, and is similar in appearance to the typical Norwood Class VII.
We feel that the early identification of the diffuse alopecia patient is important in order to screen out those who will not be surgical candidates. In addition, because the diffuse alopecias are often associated with a rather rapid progression through the four stages described, the young patient is often not emotionally prepared for this degree of hair loss, especially with DUPA. Long-term planning and careful patient counseling is, therefore, critical before any restoration should be considered. We have not yet determined the exact incidence of the diffuse androgenetic alopecias in the general male population, but they appear to be significantly more common than are the Norwood Class A’s.
It is possible that in many instances diffuse, unpatterned alopecia is not a true “androgenetic” alopecia at all but actually represents a similar pathophysiology to what has been termed “senile alopecia,”2 only occurring at a younger age. These authors evaluate the donor area for a miniaturization in every person consulted in our office for hair loss. We believe that some degree of clinically significant diffuse androgenetic alopecia occurs in a substantial number of men as they age. We have observed this in men as young as 17. Regardless of what the actual pathophysiology might prove to be, these authors believe that it is important to make a quantitative assessment of miniaturization , using densitometry, when evaluating each patient so that the physician can more accurately determine the total available supply of stable donor hair.
Treatment
We feel that the decision if and when to begin surgical treatment of the patient with Diffuse Patterned Alopecia is problematic for a number of reasons: 1) we find the patients with DPA tend to be very young, 2) the hair loss tends to progress rapidly, 3) the position of the existing frontal hairline is often unrealistically low, 4) there is a high risk of accelerated hair loss from the surgery, and 5) the patient may become extensively bald.
The physician should encourage the patient presenting with diffuse alopecia to wait as long as possible before beginning the first procedure. Delaying surgery will have a number of advantages. First, the diagnosis of Diffuse Patterned Alopecia can be more secure, so that the risk of operating on a patient who might eventuate into DUPA can be minimized. Second, waiting will enable the patient to move beyond his early “panic” phase and think clearly about whether he really wants to have a transplant which may possibly eliminate his option of wearing his hair very short if he were to become extensively bald (because of the inability to hide the donor scar). Third, because in DPA, even in the early stages, the area to be transplanted is essentially a “sea of miniaturization,” the risk of acceleration of hair loss from the surgery is much higher than in the other Norwood classes. Last, the lack of significant hairline recession makes it more difficult for the young patient to visualize and accept a hairline in a more conservative, but appropriate location.
The DPA2 patient can usually achieve a satisfactory appearance with a little more attention to styling his hair and should, therefore, not be transplanted given the risks outlined above. Patients with DPA3 are appropriate candidates as long as the transplant is aggressive with regard to the number of implants, and the planning is conservative with regard to its design. Specifically, this means that the transplant should include the front, top, and vertex in the first session, but not extend into the crown, and appropriate bitemporal recession should be built into the design, even if it is behind the patient’s existing hairline. The number of implants used should essentially be the same as if the patient was totally bald in the transplanted area, since this hair will most likely be lost in the near future. If it is anticipated that the number of implants planned in the first session will not produce a cosmetic impact at least as great as the existing hair, then the procedure should be postponed, or the risk of the procedure will outweigh the possible benefits. In addition, the implants should cover the entire area described above in one continuous unit. Although the distribution and weighting will vary depending upon the aesthetics of the hair transplant, the surgery should not be performed in sections or in multiple stages. As in the proper planning of all hair transplants, the patient must have a scalp laxity and donor density commensurate with the potential area that needs to be transplanted and must have good hair characteristics for the procedure to be worthwhile. The risk of acceleration of hair loss due to the surgery and the probability of extensive baldness must, of course, be emphasized. The DPA4 is the easiest to manage, since the risk of effluvium is gone and patient expectations are usually more realistic. These patients should be transplanted in a manner similar to the Norwood Class 6 or 7.
Conclusion
In Follicular Transplantation, large numbers of implants are used in each procedure. It is therefore critically important to accurately assess the patient’s donor reserves in the initial evaluation. We have stressed that objective measurements of density, using a densitometer, are useful in this regard, as this will not only give us specific information regarding the total number of movable hairs, but will tell us the size of the follicular units, and allow us to estimate the degree of miniaturization in both the donor and recipient areas.
In spite of the ability of the follicular transplantation procedure to move extensive quantities of implants in a single session , not all patients are good candidates for this procedure. Great care should be taken so that treatment is not begun when patients are too young or when diffuse hair loss is anticipated. The patient consultation is extremely important to be certain that the patients expectations are realistic. It is incumbent upon the physician to clearly explain to the patient what we can reasonably deliver and to honestly discuss all the limitations of the hair transplantation procedure, as well as its benefits.
When there is meticulous attention to transplanting intact follicular units and when the finite nature of the donor supply is respected, excellent cosmetic results can be achieved. With careful short and long-term planning the patients goals can often be met in one or two transplant sessions.


