
Robert M. Bernstein, M.D.
Rev. Dermatol. 2008; 3(4): 501-508
Abstract
Follicular Unit Transplantation is a powerful hair restoration technique that allows the surgeon to create very natural results. However, the ability to achieve full cosmetic benefit depends upon a number of factors including proper patient selection, accurately assessing the patient’s donor supply, appropriately designing the hair line and correctly distributing the grafts. This paper reviews the major mistakes that doctors make in these key aspects of the hair restoration process and advises the practitioner on how to avoid them so that the patient will achieve the best possible results.
Expert Commentary
Although many technical advances have been made in the field of surgical hair restoration over the past decade, particularly with the widespread adoption of follicular transplantation, many problems remain. The majority revolve around doctors recommending surgery for patients who are not good candidates. The most common reasons that patients should not proceed with surgery are that they are too young and that their hair loss pattern is too unpredictable. Young persons also have expectations that are typically too high – often demanding the density and hairline of a teenager. Many people who are in the early stages of hair loss should simply be treated with medications, rather than being rushed to go under the knife. And some patients are just not mature enough to make level-headed decisions when their problem is so emotional.
In general, the younger the patient, the more cautious the practitioner should be to operate, particularly if the patient has a family history of Norwood Class VII hair loss, or diffuse un-patterned alopecia.
Problems also occur when the doctor fails to adequately evaluate the patient’s donor hair supply and then does not have enough hair to accomplish the patient’s goals. Careful measurement of a patient’s density and other scalp characteristics will allow the surgeon to know exactly how much hair is available for transplantation and enable him/her to design a pattern for the restoration that can be achieved within those constraints.
In all of these situations, spending a little extra time listening to the patient’s concerns, examining the patient more carefully and then recommending a treatment plan that is consistent with what actually can be accomplished, will go a long way towards having satisfied patients. Unfortunately, scientific advances will improve only the technical aspects of the hair restoration process and will do little to insure that the procedure will be performed with the right planning or on the appropriate patient.
Five-year View
The improvement in surgical techniques that have enabled an ever increasing number of grafts to be placed into ever smaller recipient sites had nearly reached its limit and the limitations of the donor supply remain the major constraint for patients getting back a full head of hair. Despite the great initial enthusiasm of follicular unit extraction, a technique where hair can be harvested directly from the donor scalp (or even the body) without a linear scar, this procedure has added relatively little towards increasing the patient’s total hair supply available for a transplant. The major breakthrough will come when the donor supply can be expanded though cloning. Although some recent progress had been made in this area (particularly in animal models) the ability to clone human hair is at least 5 to 10 years away.
Key Issues
- The greatest mistake a doctor can make when treating a patient with hair loss is to perform a hair transplant on a person that is too young, as expectations are generally very high and the pattern of future hair loss unpredictable.
- Chronic sun exposure over one’s lifetime has a much more significant negative impact on the outcome of the hair transplant than peri-operative sun exposure.
- A bleeding diathesis, significant enough to impact the surgery, can be generally picked up in the patient’s history; however OTC medications often go unreported (such as non-steroidals) and should be asked for specifically.
- Depression is possibly the most common psychiatric disorder encountered in patient’s seeking hair transplantation, but it is also a common symptom of those persons experiencing hair loss. The doctor must differentiate between a reasonable emotional response to balding and a depression that requires psychiatric counseling.
- In performing a hair transplant, the physician must balance the patient’s present and future needs for hair with the present and future availability of the donor supply. It is well known that one’s balding pattern progresses over time. What is less appreciated is that the donor zone may change as well.
- The patient’s donor supply depends upon a number of factors including the physical dimensions of the permanent zone, scalp laxity, donor density, hair characteristics, and most importantly, the degree of miniaturization in the donor area – since this is a window into the future stability of the donor supply.
- Patients with very loose scalps often heal with widened donor scars.
- One should never assume that a person’s hair loss is stable. Hair loss tends to progress over time. Even patients who show a good response to finasteride will eventually lose more hair.
- The position of the normal adult male hairline is approximately 1.5 cm above the upper brow crease. Avoid placing the newly transplanted hairline at the adolescent position, rather than one appropriate for an adult.
- A way to avoid having a hair transplant with a look that is too thin is to limit the extent of coverage to the front and mid-scalp until an adequate donor supply and a limited balding pattern can be reasonably assured – an assurance that can only come after the patient ages. Until that time, it is best to avoid adding coverage to the crown.
Introduction
Hair Transplantation has been available as a treatment for hair loss for over 40 years. ((Orentreich N: Autografts in alopecias and other selected dermatological conditions. Annals of the New York Academy of Sciences 83:463-479, 1959.))
Through a majority of that time, hair transplantation was characterized by the use of plugs, slit grafts, flaps and mini-micro grafts. Although these were the best tools available to physicians at the time, they were incapable of producing consistently natural results.
With the introduction of Follicular Unit Transplantation (FUT) in 1995, doctors were finally able to produce these natural results. ((Bernstein RM, Rassman WR, Szaniawski W, Halperin A: Follicular Transplantation. Intl J Aesthetic Restorative Surgery 1995; 3: 119-32.)) But the mere capability to produce them did not necessarily ensure that these natural results would actually be achieved. The FUT procedure presented new challenges to the hair restoration surgeon and only when the procedure was properly planned and perfectly executed, would the patient truly benefit from the power of this new technique. ((Bernstein RM, Rassman WR: Follicular Transplantation: Patient Evaluation and Surgical Planning. Dermatol Surg 1997; 23: 771-84.))
The ability of follicular unit grafts to mimic nature soon produced results that were completely undetectable. This is the hallmark of Follicular Unit Hair Transplantation. ((Bernstein RM, Rassman WR: The Aesthetics of Follicular Transplantation. Dermatol Surg 1997; 23: 785-99.)) Of equal importance, however, is hair conservation – the one to one correspondence between what is harvested from the donor area and what ultimately grows in the recipient scalp. Since a finite donor supply is the main constraint in hair transplantation, the preservation of hair is a fundamental aspect of every technique. However, unlike the older procedures that used large grafts, the delicate follicular units are easily traumatized and very susceptible to desiccation, making follicular unit transplantation procedures, involving thousands of grafts, particularly challenging. ((Gandelman M, et al: Light and electron microscopic analysis of controlled injury to follicular unit grafts. Dermatol Surg 2000; 26(1): 31.))
As of this writing, the vast majority of hair transplants performed in the United States use Follicular Unit Transplant techniques. Due to limited space, this review will focus on only this technique and not on the older procedures. Nor will it focus on Follicular Unit Extraction, since this technique is still evolving and the ways to avoid the major pitfalls of this procedure are still being worked out and a subject onto itself. As the title suggests, this paper will focus on the prevention of the various problems encountered in FUT, rather than its treatment – an equally important subject, but one that has already been covered in an extensive review. ((Bernstein RM, Rassman WR, Rashid N, Shiell R: The art of repair in surgical hair restoration – Part I: Basic repair strategies. Dermatol Surg 2002; 28(9): 783-94.)), ((Bernstein RM, Rassman WR, Rashid N, Shiell R: The art of repair in surgical hair restoration – Part II: The tactics of repair. Dermatol Surg 2002; 28(10): 873-93.))
For those not familiar with Follicular Unit Transplantation, there is a concise review of the topic in the dermatology text Surgery of the Skin. ((Bernstein RM, Follicular Unit Hair Transplantation. In: Robinson JK, Hanke CW, Siegel DM, Sengelmann RD, editors: Surgery of the Skin, Elsevier Mosby, London UK. 2005.)) For more detailed information, several hair transplant textbooks have sections devoted to this technique. ((Unger WP, Shapiro R. Hair Transplantation. New York: Marcel Dekker, Inc. 2004.)), ((Bernstein RM, Rassman, WR. Follicular Unit Transplantation. In: Haber RS, Stough DB, editors: Hair Transplantation, Chapter 12. Elsevier Saunders, 2006: 91-97.))
The most common types of problems that occur in FUT procedures can be grouped into two broad categories; those involving errors in planning the hair transplant and those caused by errors in surgical technique. Of the two, errors in planning often lead to far more serious consequences for the patient and will be the subject of this paper.
Patient Selection
Age
The single greatest mistake a doctor can make when treating a patient with hair loss is performing a hair transplant on a person that is too young. Although, there is no specific age that can serve as a cut off (since this will vary from person to person), understanding the problems associated with performing hair restoration in young persons can help the physician in deciding when surgery may be appropriate. Getting it wrong can literally ruin a young person’s life.
When someone is beginning to lose hair in their teens or early 20s, there is a significant chance that he (or she) may become extensively bald later in life and that the donor area may eventually thin and become see-through over time. Although miniaturization (decreased hair shaft diameter) in the donor area is an early sign that this may occur, and can be picked up using densitometry, these changes may not be apparent when a person is still young.
If a person were to become very bald (become a Norwood Class 6 or a Class 7) then he would often not have enough hair to cover his crown. A transplanted scalp with a thin or balding crown is a pattern acceptable for an adult, but totally unsuitable for a person in his twenties. ((Norwood OT. Male pattern baldness: classification and incidence. So. Med. J 1975; 68:1359-1365.)) In addition, if the donor area were to thin over time, the donor scar might become visible if the hair were worn short – a style that is much more common in people who are young.
Expectations
This subject is very closely related to age. For surgical hair restoration to be successful, expectations must match what can actually be accomplished. The expectations of a young person are usually to return to the look they had as a teenager; namely to have a broad, flat hairline and to have all of the density they had only a few years before.
The problem is that a hair transplant neither creates more hair (and therefore can’t increase overall density) nor prevents further hair loss (so the pattern must be appropriate as the person ages). But since receded temples and a thin crown is not an acceptable look for a young person, the surgery should best be postponed in a person in whom this is not acceptable. As a person ages, he often becomes more realistic and is happy with what a hair transplant can actually achieve. And, over time, if a person’s donor area proves to be stable and his hair loss limited, more ambitious goals can be attained.
Chronic Sun Exposure
Although it is common wisdom to avoid sunburns after a hair transplant, in fact, significant chronic sun exposure over one’s lifetime has a much more significant negative impact on the outcome of the hair transplant then peri-operative sun exposure.
Actinic damage alters the collagen and elastic fibers so that the grafts are not grasped as securely and the alteration to the vasculature decreases the ability of the recipient tissue to support the transplantation of a large number of grafts. Even with the very small recipient sites used in follicular unit transplantation, making sites too close can result in a compromised blood supply and result in poor growth.
Another issue is that a hair transplant will cover areas of sun damage and make cancer detection more difficult. When the actinic related growths are finally treated, the involved sections of the hair transplant will be destroyed.
The best approach in a person with significant sun damage is to first treat the entire scalp aggressively with 5-flurouracil to remove all of the pre-cancerous lesions before hair transplant is contemplated. One should wait at least 6-12 months after the treatment for the scalp to completely heal, as the tissue will be more friable during this period. Although this treatment can set the surgery back a year or more, it will result in better graft survival and less problems with future skin cancer detection.
Medical Conditions and Medications
Although not necessarily an absolute contraindication to surgery, a number of medical conditions make the follicular unit hair transplant procedure more problematic and need to be taken into account. Whenever significant medical conditions are present, it is always prudent to obtain medical clearance from the patient’s primary care physician or appropriate specialist.
Because the scalp is quite vascular, and FUT procedures involve a large surgical team, patients that are known to have blood born pathogens, such as HIV and Hepatitis B and C, pose some increased risk to the staff, despite the fact that universal precautions are used. It is useful if the team is aware of the medical histories of hair transplant patients so that they can proceed with a higher degree of alert when necessary.
In an HIV positive patient, it is important to make certain that the patient’s immune status is adequate, so that the patient does not have a greater risk of infection. In patient’s with Hepatitis, it is important to assess their liver function so that the dosing of medications is appropriate.
Patients with diabetes mellitus may be at greater risk of having a peri-operative infection. In this case the normal aseptic conditions that most hair transplants are performed under might be changed to a modified sterile technique (modified in that it is difficult to prep the scalp). This should also be considered in patients with cardiac valvular disease, implanted devices and others in whom bacterial seeding might have more severe consequences. Antibiotic coverage should also be administered in high risk individuals, although it is not needed in routine hair restoration procedures. ((Haas AF, Grekin RC: Antibiotic prophylaxis in dermatologic surgery. J Am Acad Dermatol 1995; 32: 155-76.))
A bleeding diathesis, significant enough to impact the surgery, can be generally picked up in the patient’s history; however medications often go under the radar and should be asked for specifically. Patient’s often don’t think to report taking aspirin and this must be asked about as well as other non-steroidal anti-inflammatory medications. Plavix, in particular can significantly increase bleeding during the procedure. Alcohol, of course increases bleeding as well. ((Otley CC. Perioperative evaluation and management in dermatologic surgery. J Am Acad Dermatol 2006; 54: 119-27.))
One should make adjustments in a patient’s anti-coagulant medication in conjunction with his/her cardiologist or regular physician. As a general rule, one should stop anti-platelet medications one week prior to the hair transplant, but the interval will vary depending upon the specific drug, the size of the procedure, and the importance of the medication to the patient’s health. They can be resumed three days after the procedure. If the anticoagulants cannot be stopped, it may be reasonable to proceed with a smaller session.
Since epinephrine is used in most hair restoration procedures, if a person has a history of arrhythmias or other cardiac disease that could be exacerbated by epinephrine, medical clearance from the patient’s primary care doctor, or cardiologist, should be obtained. Epinephrine can also interact with broad-beta blocking agents such as propranolol, causing a hypertensive crisis; therefore, it is best to have the patient switch to a selective beta-blocker for the surgery. ((Gandelman M, Bellio R, Barretto M: Beta-blockers and local anesthetics with vasoconstrictors: A dangerous association. Intl J Aesthetic Restorative Surgery 1995; 3 (2): 143-45.))
A number of manipulations can be used during the procedure to control bleeding and decrease the need for epinephrine. Among the most useful, is to scatter the recipient sites broadly over the area to be transplanted (allowing the extrinsic pathway to begin coagulation) and then filling in the areas with additional sites when the bleeding has subsided. ((Bernstein RM, Rassman WR: Limiting epinephrine in large hair transplant sessions. Hair Transplant Forum International 2000; 10(2): 39-42.))
If patients have a history of seizures, it is important that they do not discontinue their medication for the procedure and that medical clearance is obtained. One should also remember that otherwise normal patients can have a vaso-vagal episode during the procedure; particularly during the administration of the local anesthetic. This can be avoided by immediately placing the patient in Trendelenberg as soon as the patient complains of nausea or begins to sweat, or look pale.
A patient should be monitored with a pulse oximiter if a significant amount of sedatives or other respiratory depressants are used. The patient should be monitored closely to be sure that local anesthetics are administered in safe amounts and that the warning signs of lidocaine overdose are well known to all members of the surgical team. ((Skidmore RA, Patterson JD, Tomsick, RS: Local anesthetics. Dermatol Surg 1996; 22:511-522.))
Finally, it is helpful to have a pre-printed summary of all the medications and their doses commonly used during the procedure. This can be given to the patient’s regular physician when seeking medical clearance.
Psychological Factors
Hair loss can take a psychological toll on a person’s self-esteem and cause considerable emotional distress. When a person has underlying psychiatric issues, the impact can be more severe and, therefore, management of hair loss considerably more difficult. It is important to identify these problems as well as other psychological factors that may play a role in a patient’s ability to clearly understand both the hair restoration process and its anticipated outcome.
In some cases, counseling can be done in conjunction with hair restoration, but often it should precede treatment, especially when surgery is contemplated. It is prudent to obtain clearance for surgery from a psychiatrist or clinical psychologist when there is a history of mental illness, or when it is suspected at the time of the consultation.
A number of psychiatric conditions are particularly relevant to the successful outcome of a hair transplant. These include Trichotillomania, Obsessive-Compulsive Disorder (OCD), Body Dysmorphic Syndrome (BDS), and Depression.
Trichotillomania is a relatively common condition characterized by the persistent urge to pull out one’s hair. It most commonly involves scalp hair, but can also involve the eyelashes, facial hair or other body hair. It often results in bald patches and can be identified by short hairs in the affected area that are not long enough to grasp. Active trichitollomania on any part of the body is an obvious contraindication to a hair transplant, but if a person has a history of this condition, the doctor should also be cautious and only consider surgery if the therapist is confident that the condition has little chance of recurring.
Obsessive-compulsive disorder (OCD) is a condition characterized by recurrent, intrusive thoughts (obsessions) and related behaviors (compulsions) which attempt to neutralize the anxiety or stress caused by the obsessions. In consultation, the OCD patient often asks a litany of questions and often asks the next question before listening to the answer to previous one. OCD patients are extremely difficult to satisfy and even in a very successful hair transplant can focus on a minor imperfection seeming oblivious to the good overall result.
Body dysmorphic disorder (BDD) is a mental disorder that involves a distorted image of one’s body. The person is extremely critical of their physical self, despite the fact there may be no actual defect. It should be obvious that patients with BDD will not be satisfied with a hair transplant, or other forms of cosmetic procedures, and the condition is best treated by a psychiatrist rather than a surgeon. Another note of caution is that patients with BDD have a much higher suicide rate than the general population, even greater than patients with depression. ((Phillips KA, Menard W: Suicidality in body dysmorphic disorder: A prospective study. Am J Psychiatry, 2006; 163:1280-82.))
Depression is possibly the most common psychiatric disorder encountered in patient’s seeking hair transplantation, but it is also a common symptom of those experiencing hair loss. The doctor must differentiate between a reasonable emotional response to balding and a depression that requires psychiatric counseling. It is important to realize that a hair transplant will be ineffective in curing a medical depression and unfulfilled expectations may lead to a worsening of the condition.
Patient Assessment
Donor Supply
In performing a hair transplant, the physician must balance the patient’s present and future needs for hair with the present and future availability of the donor supply. It is well known that one’s balding pattern progresses over time. What is less appreciated is that the donor zone may change as well.
The patient’s donor supply depends upon a number of factors including the physical dimensions of the permanent zone, scalp laxity, donor density, hair characteristics, and most importantly, the degree of miniaturization in the donor area – since this is a window into the future stability of the donor supply.
The size of the donor area is determined by both its width (height) and its length. When assessing the potential width of the donor area, doctors usually assess the lowermost point that the balding will reach, i.e. the top part of the permanent zone. However, it is equally important to pay attention to the inferior margin as well. It is common for the hair to thin significantly at the nape of the neck as a person ages, producing an “ascending hairline.” Since this can significantly diminish the width of the donor area, any evidence that this process may occur should be taken into account in the planning. Loss of the temporal points is another process that has a significant impact on the donor supply. Not only does it foreshorten the potential length of the donor strip but it often portends very significant baldness.
Scalp laxity is another variable that affects the amount of available donor hair. Very tight scalps significantly limit the amount of donor hair that can be removed through strip harvesting. The constraint imposed by a tight scalp is not always apparent in the first session, but can plague the hair restoration down the line; therefore, it should be evaluated carefully in the initial patient assessment. A very loose scalp can present its own set of problems, as patients with very loose scalps often heal with widened donor scars. ((Bernstein RM, Rassman WR. The scalp laxity paradox. Hair Transplant Forum International 2002; 12(1): 9-10.))
The average donor density of a Caucasian is about 225 hairs/cm2. This can easily be measured using a hand-held instrument called a densitometer. (2) When the density of a Caucasian is below 180, a hair transplant should be undertaken with great caution. In this author’s opinion, when the maximum donor density is below 150/hair mm2, a person should generally not be transplanted, as there will not be enough donor hair to make the procedure cosmetically worthwhile and the risk of a visible donor scar is too great. (3) Exceptions would be an older person with very limited expectations and in races where the normal density is lower (i.e. Asians and Africans).
Hair characteristics, particularly hair shaft diameter, are as important as the absolute number of hairs in determining the outcome of a procedure. The amount of transplantable hair is related to both the number of movable hairs (determined by the size of the donor area, scalp laxity and donor density), multiplied by the hair shaft cross sectional area. Since each hair in a person with coarse hair can have over 5 times the volume as a person with fine hair, the estimate (or actual measurement) of hair shaft diameter is important in determining the overall donor supply.
Miniaturization, the progressive diminution of hair shaft diameter and length (the result of the action of DHT on the hair follicle) produces thinning on the front, top and crown of the scalp and is the hallmark of androgenetic alopecia. But the back and sides of the scalp can miniaturize as well and when a significant portion of a patient’s donor area is miniaturized, the hair in this area can be rendered useless for a hair transplant. (Figures 1 and 2)
This condition, called diffuse unpatterned hair loss (or DUPA), is the most common type of hair loss seen in women and it is not uncommon in men. It goes without saying, that every patient, male or female, in whom a transplant is being considered, should be evaluated for donor miniaturization using densitometry to make sure that the donor hair to be transplanted is stable.
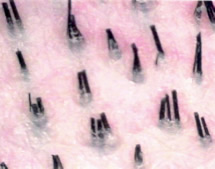
Figure 1. Normal density of 2.2 hairs/mm2
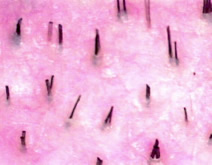
Figure 2. Low density (1.3 hairs/mm2) and extensive miniaturization.
Recipient Demand
One should never assume that a person’s hair loss is stable. Hair loss tends to progress over time. Even patients who show a good response to finasteride will eventually lose more hair. It is always best to consider the reasonable worst-case scenario when assessing how bald the patient may become, so that the finite donor hair can be allocated properly. Although the Norwood classification is very helpful in staging the hair loss, it doesn’t take into account actual scalp dimensions. Just like the donor site, the recipient area should actually be measured. Even within a single Norwood class, there is a vast difference between a patient with a narrow forehead and one with a very broad head with respect to the actual surface that needs to be covered, and thus the number of grafts required for the restoration.
Designing the Hairline
Hairline Position
In the adolescent, the hairline sits just above the upper brow crease formed by the upper border of the frontalis muscle directly below it. The position of the normal adult male hairline is approximately 1.5cm above this crease at the midline). A common error is to place the newly transplanted hairline at the adolescent position, rather than one appropriate for an adult. Although the younger patient, first experiencing hair loss, may put considerable pressure on the doctor to place hair in the lower position, the physician should not yield to this demand.
Under normal circumstances, as a patient ages, his density decreases and the natural hairline will move back somewhat. However, a transplanted hairline is immutable. Therefore, when the transplanted patient continues to thin or bald (which he invariable will) the fixed low frontal hairline will begin to look out of place, since it is natural for a person with decreased overall hair volume to have a slightly receded hairline, rather than one that is still in the adolescent position.
Hairline Shape
A similar logic applies when choosing the shape of the hairline. As a male passes from adolescence to adulthood, his broad, flat hairline evolves into a more tapered shape with some recession at the temples. A persistent low, broad hairline is enjoyed by those who also maintain their adolescent density. This situation is not present in those who are suffering from androgenetic alopeica; therefore, a transplanted flat hairline will not “age well” over time and will look unnatural as the patient’s overall density decreases and particularly as the crown begins to thin.
If a person is older, has maintained a high donor density, and has a small risk of extensive hair loss, a broader hairline is possible. However, this is not this case for the person who is starting to bald at a young age, since he has a significant risk of extensive baldness and, more importantly, the extent of his future hair loss can not be known at the time the surgery is planned.
Graft Distribution
The nuances of graft distribution and the multitude of problems that result from distributing grafts improperly are beyond the scope of this writing; however, there are two main but related themes that the hair transplant surgeon should be cognizant of when deciding where to place grafts. The first is to set a target area of coverage that takes into account the patient’s future balding pattern, as well as, his total donor hair supply. The second is to forward weight the grafts, rather than distributing them evenly over the top of the scalp.
Extent of Coverage
The problem of deciding how much bald scalp a hair transplant should cover can be illustrated as follows. As an example, take a patient whose total number of follicular unit grafts available to harvest is around 5,500. The front part of the scalp has a surface area of about 50 cm2. The top or mid-scalp has an area of about 150 cm2 and the vertex or crown about 175 cm2 (Figure 3). However, the size of the bald crown can vary dramatically depending upon the extent of hair loss, reaching over 200 cm2 in a Norwood Class VII patient.
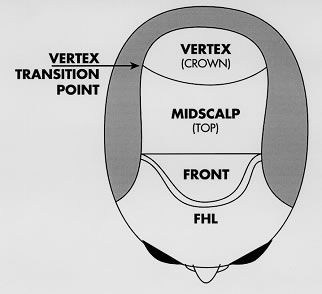
Figure 3. Regions of the scalp
If the front and top of the scalp were transplanted using all of the patients donor hair, the transplanted density would be only 5,500 grafts/200 cm2 or 27.5 grafts/cm2 (less than 1/3 the density of the patient’s original hair). If the crown were covered as well, that would be 5,500 grafts/400cm2 or 12.5 grafts/cm2 (only 15% the density of the patient’s original hair). Using various manipulations, such as creating different densities in different parts of the scalp, a skilled surgeon can make 1/3 of the overall density look like a substantial amount of hair. However, working with only 15% of the original density, can make the job of creating a natural look significantly more difficult, if not impossible.
The way to avoid having a hair transplant with a look that is too thin, or see-through, is to limit the extent of coverage to the front and mid-scalp until an adequate donor supply and a limited balding pattern can be reasonably assured – an assurance that can only come after the patient ages. Until that time, it is best to avoid adding coverage to the crown.
Another problem with transplanting the crown early is that as the crown expands additional hair will be needed to follow the expanding area of baldness outward, just to keep the first hair transplant looking natural. This may require considerable amounts of hair that will not be available to cover the front and mid-scalp if that were too bald as well. On the other hand, if the hair transplant was limited to the vertex transition point or VTP (see figure above), the restoration would look natural without further surgery no matter how far the hair loss in the crown progressed. The reason is that the front and top of the scalp represent a complete cosmetic unit, with the VTP as the natural posterior boundary – so it is natural for hair to cover this region of the scalp but not beyond.
Density Gradients
Another way for surgeons to prevent a thin, see-through look is to avoid distributing the grafts evenly over the transplanted area. It goes without saying that only 1-hair grafts should be used at the hairline, with larger grafts behind them, but there are additional ways to produce the gradations of density to mimic the way hair grows in nature. Specifically, the greatest density should be in the front part of the scalp (shown in brown) and particularly in the frontal forelock area (shown in dark brown). (Figure 4.).
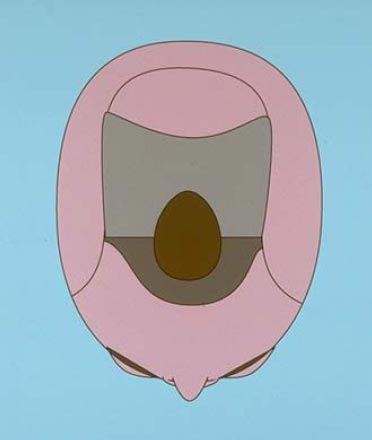
Figure 4. The frontal region of the scalp (brown) and the frontal forelock area (dark brown)
The greater density in the front of the scalp forelock area can be created in two ways; by placing the recipient sites closer together in this location and by using larger follicular units in the area (i.e. 3- and 4- hair units rather than 1s and 2s). These techniques may be use in combination to achieved greater density but, as will be discussed in the following section, if done to excess, may compromise growth.
Summary
Follicular unit transplantation is a powerful hair restoration technique that allows the surgeon to create natural hair patterns and produce results that mimic nature. The success of the procedure depends greatly on proper patient selection, accurately assessing the patient’s donor supply, and distributing the grafts in a way that is appropriate for a person who will continue to age and eventually thin over time. With thoughtful planning, major mistakes can be avoided and our patients will be able to achieve the full benefit of this remarkable procedure.


